

Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis
- PMID: 18427090
- PMCID: PMC2292779
- DOI: 10.1503/cmaj.071802
Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis
Abstract
Background: Mechanical ventilation in the prone position is used to improve oxygenation in patients with acute hypoxemic respiratory failure. We sought to determine the effect of mechanical ventilation in the prone position on mortality, oxygenation, duration of ventilation and adverse events in patients with acute hypoxemic respiratory failure.
Methods: In this systematic review we searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials and Science Citation Index Expanded for articles published from database inception to February 2008. We also conducted extensive manual searches and contacted experts. We extracted physiologic data and clinically relevant outcomes.
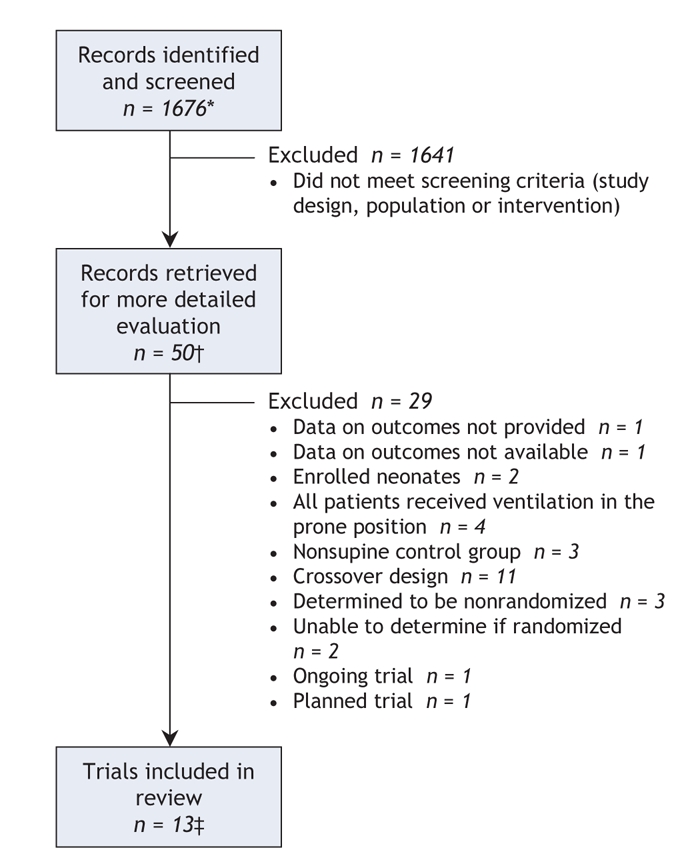
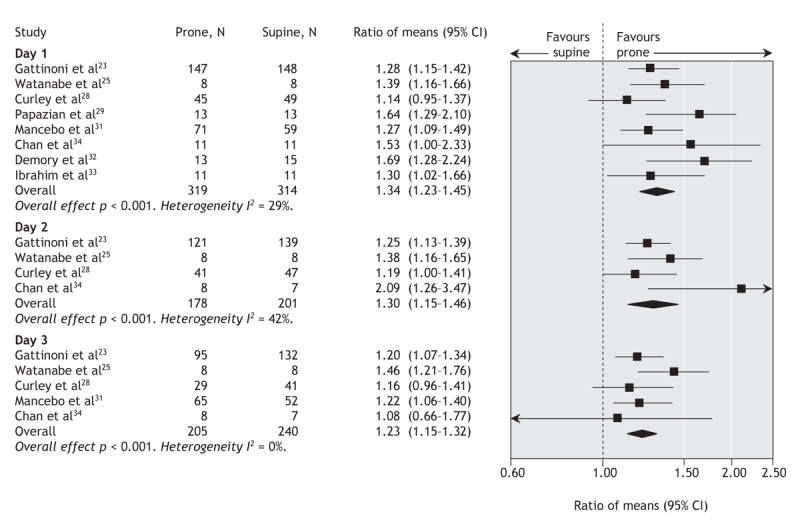
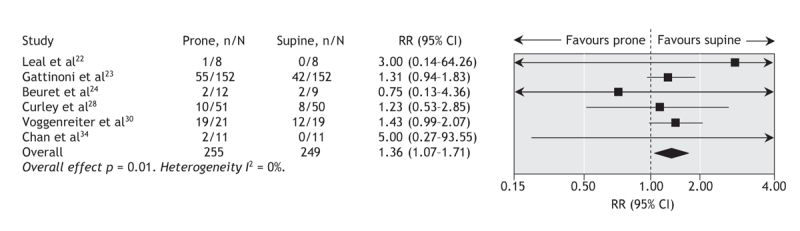
Results: Thirteen trials that enrolled a total of 1559 patients met our inclusion criteria. Overall methodologic quality was good. In 10 of the trials (n = 1486) reporting this outcome, we found that prone positioning did not reduce mortality among hypoxemic patients (risk ratio [RR] 0.96, 95% confidence interval [CI] 0.84-1.09; p = 0.52). The lack of effect of ventilation in the prone position on mortality was similar in trials of prolonged prone positioning and in patients with acute lung injury. In 8 of the trials (n = 633), the ratio of partial pressure of oxygen to inspired fraction of oxygen on day 1 was 34% higher among patients in the prone position than among those who remained supine (p < 0.001); these results were similar in 4 trials on day 2 and in 5 trials on day 3. In 9 trials (n = 1206), the ratio in patients assigned to the prone group remained 6% higher the morning after they returned to the supine position compared with patients assigned to the supine group (p = 0.07). Results were quantitatively similar but statistically significant in 7 trials on day 2 and in 6 trials on day 3 (p = 0.001). In 5 trials (n = 1004), prone positioning was associated with a reduced risk of ventilator-associated pneumonia (RR 0.81, 95% CI 0.66-0.99; p = 0.04) but not with a reduced duration of ventilation. In 6 trials (n = 504), prone positioning was associated with an increased risk of pressure ulcers (RR 1.36, 95% CI 1.07-1.71; p = 0.01). Most analyses found no to moderate between-trial heterogeneity.
Interpretation: Mechanical ventilation in the prone position does not reduce mortality or duration of ventilation despite improved oxygenation and a decreased risk of pneumonia. Therefore, it should not be used routinely for acute hypoxemic respiratory failure. However, a sustained improvement in oxygenation may support the use of prone positioning in patients with very severe hypoxemia, who have not been well-studied to date.
Figures


Comment in
-
Ventilation in the prone position: for some but not for all?CMAJ. 2008 Apr 22;178(9):1174-6. doi: 10.1503/cmaj.080359. CMAJ. 2008. PMID: 18427093 Free PMC article. No abstract available.
References
-
- Bernard GR, Artigas A, Brigham KL, et al. The American–European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994;149:818-24. - PubMed
-
- Artigas A, Bernard GR, Carlet J, et al. The American–European Consensus Conference on ARDS, part 2: Ventilatory, pharmacologic, supportive therapy, study design strategies, and issues related to recovery and remodeling. Acute respiratory distress syndrome. Am J Respir Crit Care Med 1998;157:1332-47. - PubMed
-
- Derdak S, Mehta S, Stewart TE, et al. High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: a randomized, controlled trial. Am J Respir Crit Care Med 2002;166:801-8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous