

Granulocyte-macrophage colony-stimulating factor potentiates rituximab in patients with relapsed follicular lymphoma: results of a phase II study
- PMID: 18427151
- PMCID: PMC2443403
- DOI: 10.1200/JCO.2007.13.7729
Granulocyte-macrophage colony-stimulating factor potentiates rituximab in patients with relapsed follicular lymphoma: results of a phase II study
Abstract
Purpose: We hypothesized that granulocyte-macrophage colony-stimulating factor (GM-CSF) could potentiate the clinical activity of rituximab given its individual and cooperative effects on Fc gamma RIIa- and Fc gamma RIIIa-expressing cells. A phase II clinical study combining GM-CSF and rituximab was initiated in patients with relapsed follicular lymphoma (FL) to determine the clinical and biologic responses, as well as safety of the combination.
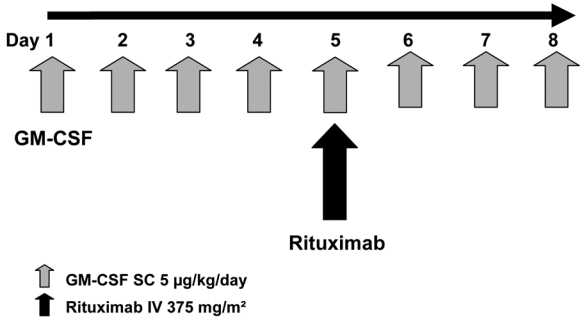
Patients and methods: Thirty three patients with relapsed FL were treated with GM-CSF 5 microg/kg/d on days 1 to 8 and rituximab 375 mg/m(2) on day 5 of each 21-day cycle for four cycles. Clinical response and tolerability were examined according to international criteria. Biologic monitoring included evaluation of immune cells involved in rituximab activity.
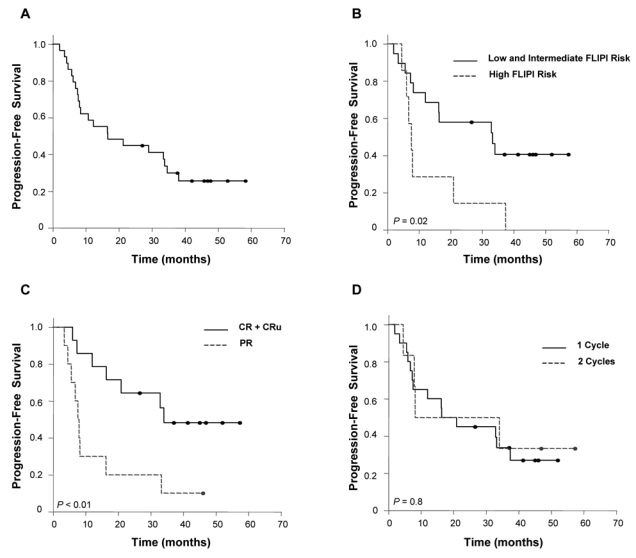
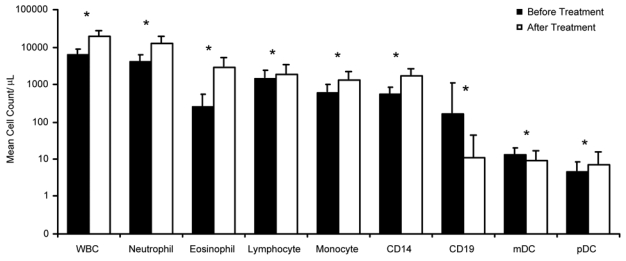
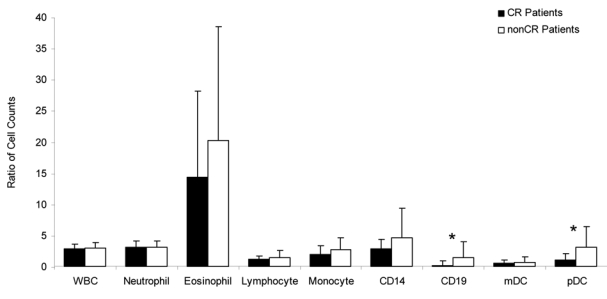
Results: Of 33 evaluated patients, a 70% overall response rate (complete response plus complete response unconfirmed, 45%) and a median progression-free survival (PFS) of 16.5 months were achieved. Outcome was influenced by the quality of response and the Follicular Lymphoma International Prognostic Index (FLIPI), where low- and intermediate-risk FLIPI groups were associated with significantly better PFS. After treatment there was a significant increase in granulocyte and monocyte counts. Examination of dendritic cell response showed an overall increase in plasmacytoid dendritic cells, especially in non-complete response patients, after treatment. Addition of GM-CSF did not impair tolerance to rituximab, and adverse events were rare and mild.
Discussion: GM-CSF plus rituximab results in high response rates, along with a tolerable safety profile in patients with relapsed or progressive FL. The improved efficacy over rituximab monotherapy may be due to increases seen in monocyte, granulocyte, and dendritic cell populations.
Figures
Comment in
-
Measuring granulocyte and monocyte accumulation at malignant lymphoma sites.J Clin Oncol. 2009 Jan 1;27(1):154-5. doi: 10.1200/JCO.2008.19.2393. Epub 2008 Nov 24. J Clin Oncol. 2009. PMID: 19029411 No abstract available.
References
-
- Armitage JO, Weisenburger DD. New approach to classifying non-Hodgkin’s lymphomas: clinical features of the major histologic subtypes: Non-Hodgkin’s Lymphoma Classification Project. J Clin Oncol. 1998;16:2780–2795. - PubMed
-
- Reff ME, Garner K, Chambers KS, et al. Depletion of B cells in vivo by a chimeric mouse human monoclonal antibody to CD20. Blood. 1994;83:435–445. - PubMed
-
- McLaughlin P, Grillo-Lopez AJ, Link BK, et al. Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: Half of patients respond to a four-dose treatment program. J Clin Oncol. 1998;16:2825–2833. - PubMed
-
- van Oers MH, Klasa R, Marcus RE, et al. Rituximab maintenance improves clinical outcome of relapsed/resistant follicular non-Hodgkin lymphoma in patients both with and without rituximab during induction: results of a prospective randomized phase 3 intergroup trial. Blood. 2006;108:3295–3301. - PubMed
-
- Forstpointner R, Unterhalt M, Dreyling M, et al. Maintenance therapy with rituximab leads to a significant prolongation of response duration after salvage therapy with a combination of rituximab, fludarabine, cyclophosphamide and mitoxantrone (R-FCM) in patients with relapsed and refractory follicular and mantle cell lymphomas - results of a prospective randomized study of the German low grade lymphoma study group (GLSG) Blood. 2006;108:4003–4008. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
