

Rapid scaling-up of antiretroviral therapy in 10,000 adults in Côte d'Ivoire: 2-year outcomes and determinants
- PMID: 18427206
- PMCID: PMC3921665
- DOI: 10.1097/QAD.0b013e3282f768f8
Rapid scaling-up of antiretroviral therapy in 10,000 adults in Côte d'Ivoire: 2-year outcomes and determinants
Abstract
Objective: To assess the rates and determinants of mortality, loss to follow-up and immunological failure in a nongovernmental organization-implemented program of access to antiretroviral treatment in Côte d'Ivoire.
Methods: In each new treatment center, professionals were trained in HIV care, and a computerized data system was implemented. Individual patient and program level determinants of survival, loss to follow-up and immunological failure were assessed by multivariate analysis.
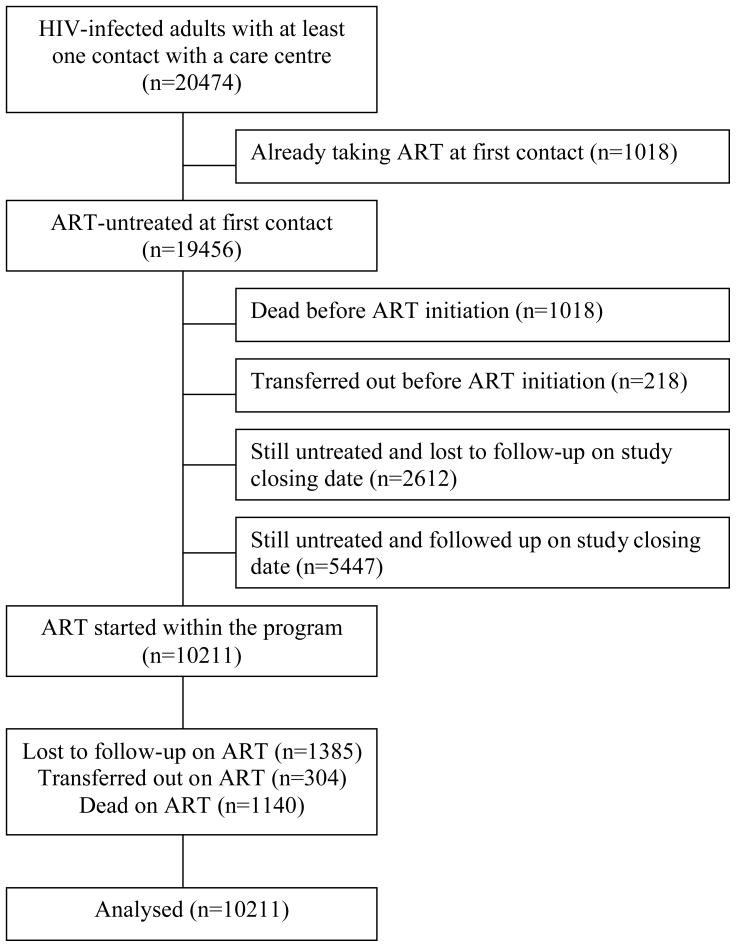
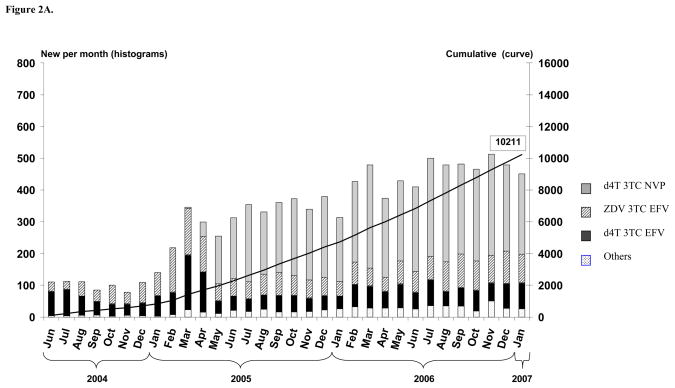
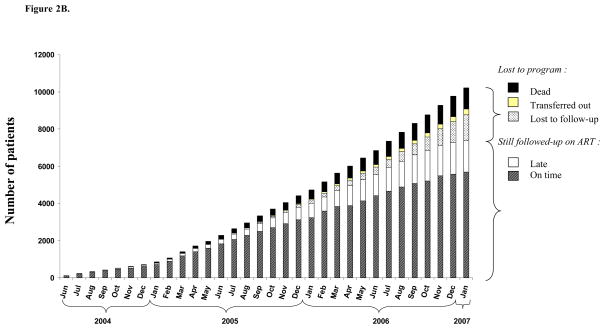
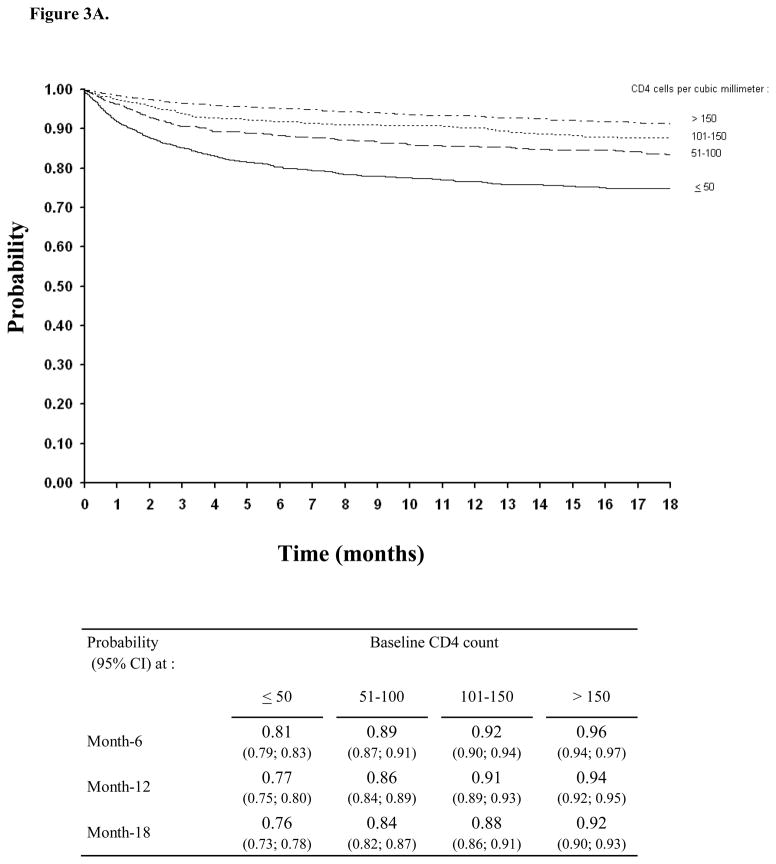
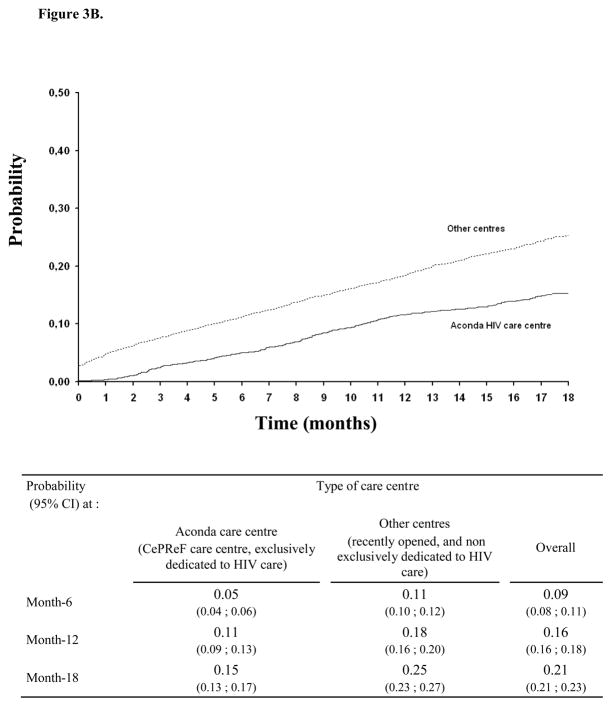
Results: Between May 2004 and February 2007, 10,211 patients started antiretroviral treatment in 19 clinics (median preantiretroviral treatment CD4 cell count, 123 cells/microl; initial regimen zidovudine-lamivudine-efavirenz, 20%; stavudine-lamivudine-efavirenz, 22%; stavudine-lamivudine-nevirapine, 52%). At 18 months on antiretroviral treatment, the median gain in CD4 cell count was +202 cells/microl, the probability of death was 0.15 and the probability of being loss to follow-up was 0.21. In addition to the commonly reported determinants of impaired outcomes (low CD4 cell count, low BMI, low hemoglobin, advanced clinical stage, old age and poor adherence), two factors were also shown to independently jeopardize prognosis: male sex (men vs. women: hazard ratio = 1.52 for death, 1.27 for loss to follow-up, 1.31 for immunological failure); and attending a recently opened clinic (inexperienced vs. experienced centers: hazard ratio = 1.40 for death, 1.58 for loss to follow-up). None of the three outcomes was associated with the drug regimen.
Discussion: In this rapidly scaling-up program, survival and immune reconstitution were good; women and patients followed up in centers with longer experience had better outcomes; outcomes were similar in zidovudine/stavudine-based regimens and in efavirenz/nevirapine-based regimens. Decreasing the rate of loss to follow-up should now be the top priority in antiretroviral treatment rollout.
Conflict of interest statement
None
Figures
References
-
- WHO/UNAIDS/UNICEF. Towards Universal Access. Scaling up priority HIV/AIDS interventions in the health sector. Progress Report. 2007 Apr; Available at: http://www.who.int/hiv/mediacentre/universal_access_progress_report_en.pdf.
-
- Anglaret X, Messou E, Ouassa T, Toure S, Dakoury-Dogbo N, Combe P, et al. Pattern of bacterial diseases in a cohort of HIV-1 infected adults receiving cotrimoxazole prophylaxis in Abidjan, Cote d’Ivoire. AIDS. 2003;17:575–584. - PubMed
-
- Gueye A, Seyler C. Case study country – Cote d’Ivoire. “Strategies for Building National-Scale Longitudinal Patient Monitoring Systems for HIV Treatment and Care in PEPFAR Countries” Workshop; October 2–5, 2007; Lusaka, Zambia. Available at: http://www.globalhivevaluation.org/meetings/zambia2007/Agenda.aspx.
-
- Rouet F, Ekouevi DK, Inwoley A, Chaix ML, Burgard M, Bequet L, et al. Field evaluation of a rapid human immunodeficiency virus (HIV) serial serologic testing algorithm for diagnosis and differentiation of HIV type 1 (HIV-1), HIV-2, and dual HIV-1-HIV-2 infections in West African pregnant women. J Clin Microbiol. 2004;42:4147–53. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
