

A reconsideration of anterior chamber flare and its clinical relevance for children with chronic anterior uveitis (an American Ophthalmological Society thesis)
- PMID: 18427621
- PMCID: PMC2258136
A reconsideration of anterior chamber flare and its clinical relevance for children with chronic anterior uveitis (an American Ophthalmological Society thesis)
Abstract
Purpose: To gain a better understanding of laser flare photometry values ("flare") as a feature of chronic anterior uveitis in children; to identify relationships between flare and other patient and disease characteristics; to describe changes in flare during course of disease; and specifically to determine whether elevated flare is predictive of subsequent adverse events.
Methods: A retrospective review of medical records was performed for all children (aged < or =16 years at disease onset) with chronic anterior uveitis presumed to be noninfectious, who were examined by one clinician at the Jules Stein Eye Institute since laser flare photometry became available at that facility. All involved eyes were studied. Cross-sectional analysis compared initial flare to other characteristics. Relationships between potential risk factors and outcomes were studied by Kaplan-Meier analyses and Cox proportional hazards regression models.
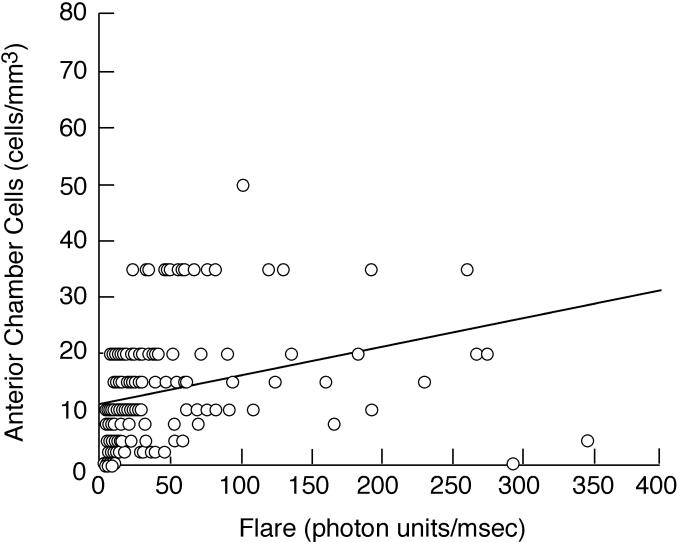
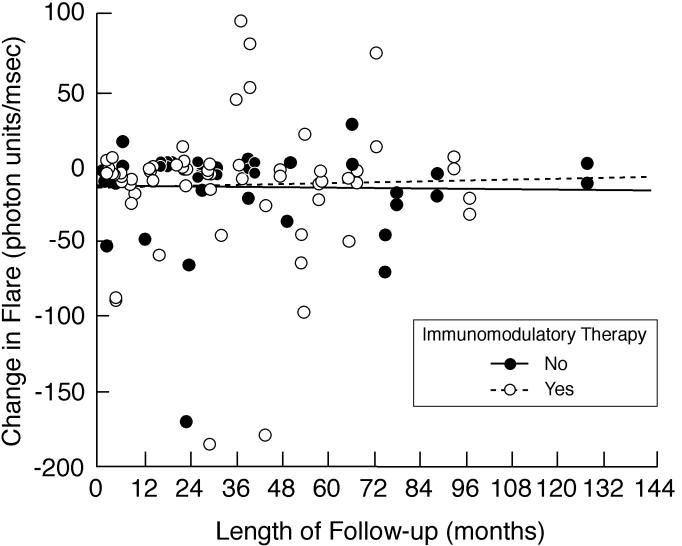
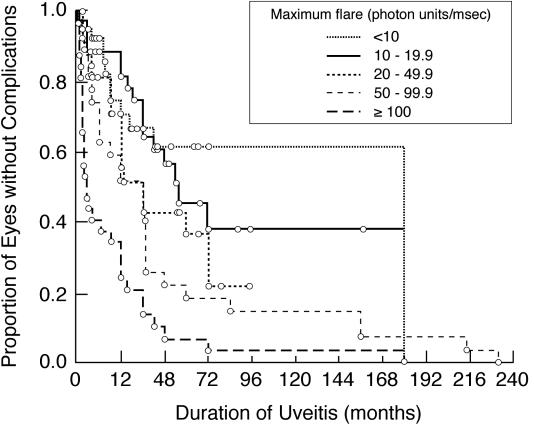
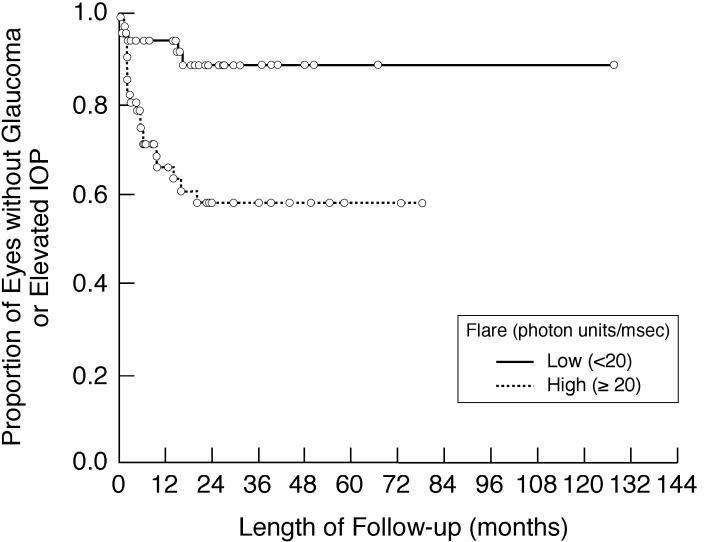
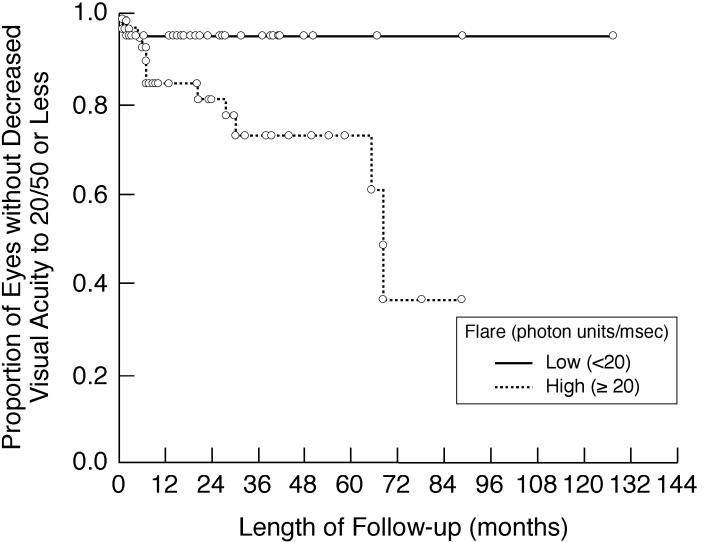
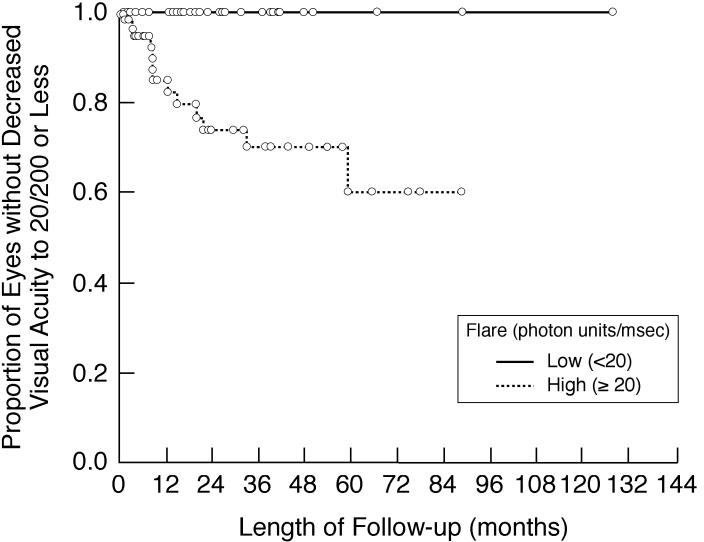
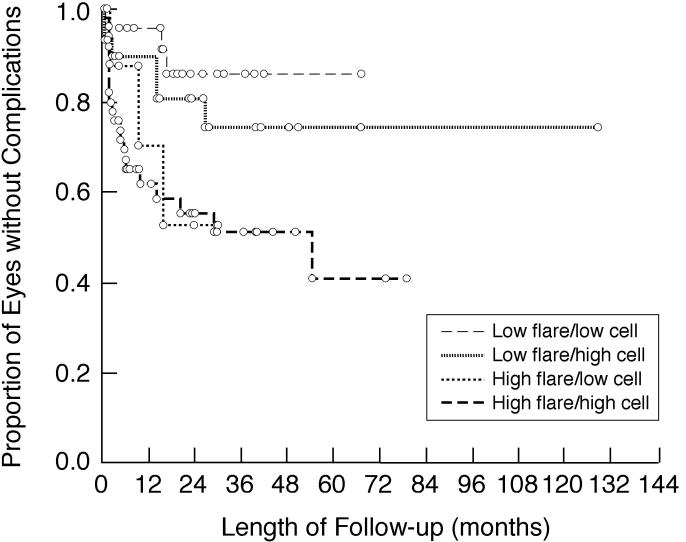
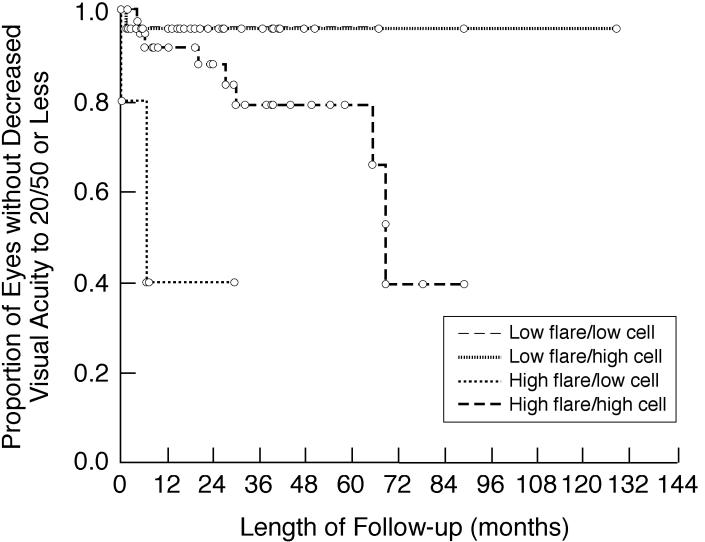
Results: Included were 114 patients (198 involved eyes). Follow-up ranged from 0 to 154.8 months (median, 23.5 months for 82 patients with follow-up). Flare was related to the following factors: anterior chamber cells, keratic precipitates, papillitis, and various complications of uveitis, including band keratopathy, posterior synechiae, and cataract. Flare was not a function of disease duration. High flare was associated with an increased risk of vision loss and development of new vision-threatening complications, including glaucoma/increased intraocular pressure, during follow-up; risk was independent of anterior chamber cells.
Conclusions: Flare may be useful in the evaluation and management of chronic anterior uveitis in children. Flare is a marker of disease severity and is predictive of adverse events during the course of disease.
Figures

References
-
- Hogan MJ, Kimura SJ, Thygeson P. Signs and symptoms of uveitis. I. Anterior uveitis. Am J Ophthalmol. 1959;47:155–170. - PubMed
-
- Duke-Elder S, Perkins ES. The clinical signs and symptoms of uveitis. In: Duke-Elder S, editor. System of Ophthalmology. St Louis: CV Mosby; 1966. pp. 132–150.
-
- Schlaegel TF. Essentials of Uveitis. 1. Boston: Little, Brown; 1967. p. 7.
-
- Smith RE, Nozik RA. Uveitis. A Clinical Approach to Diagnosis and Management. 2. Balitmore: Williams & Wilkins; 1989. Signs of uveitis; pp. 16–17.
-
- Whitcup SM. Examination of the patient with uveitis. In: Nussenblatt RB, Whitcup SM, editors. Uveitis. Fundamentals and Clinical Practice. 3. Philadelphia: Mosby; 2004. pp. 57–69.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
