

Cost-related medication nonadherence and spending on basic needs following implementation of Medicare Part D
- PMID: 18430911
- PMCID: PMC3781951
- DOI: 10.1001/jama.299.16.1922
Cost-related medication nonadherence and spending on basic needs following implementation of Medicare Part D
Abstract
Context: Cost-related medication nonadherence (CRN) has been a persistent problem for individuals who are elderly and disabled in the United States. The impact of Medicare prescription drug coverage (Part D) on CRN is unknown.
Objective: To estimate changes in CRN and forgoing basic needs to pay for drugs following Part D implementation.
Design, setting, and participants: In a population-level study design, changes in study outcomes between 2005 and 2006 before and after Medicare Part D implementation were compared with historical changes between 2004 and 2005. The community-dwelling sample of the nationally representative Medicare Current Beneficiary Survey (unweighted unique n = 24,234; response rate, 72.3%) was used, and logistic regression analyses were controlled for demographic characteristics, health status, and historical trends.
Main outcome measures: Self-reports of CRN (skipping or reducing doses, not obtaining prescriptions) and spending less on basic needs to afford medicines.
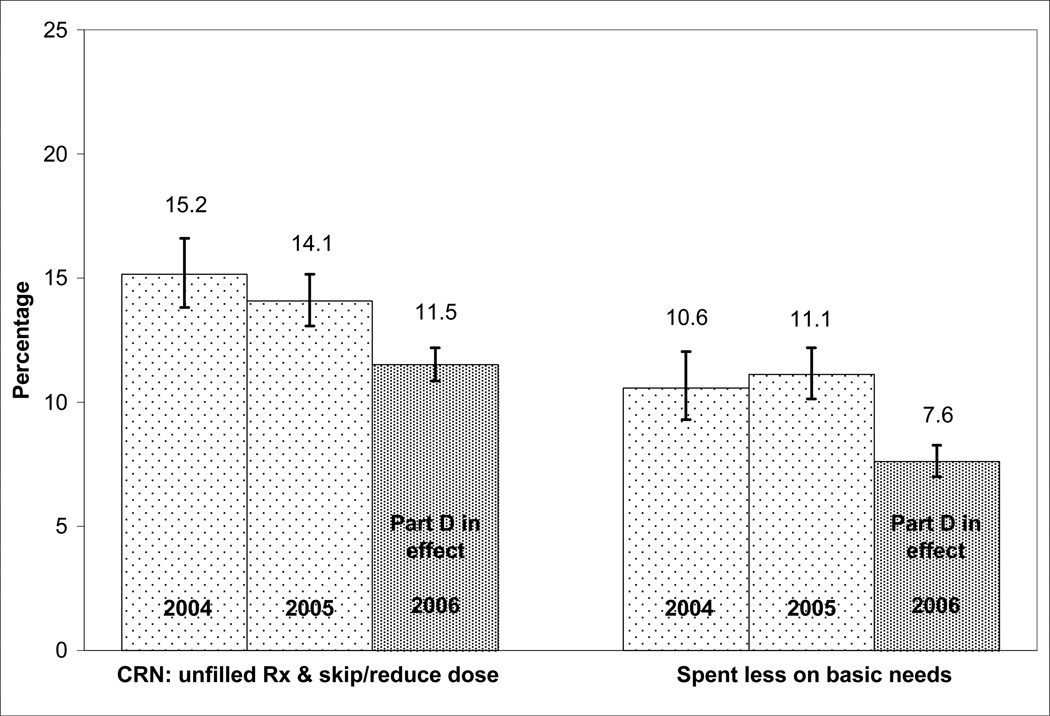
Results: The unadjusted, weighted prevalence of CRN was 15.2% in 2004, 14.1% in 2005, and 11.5% after Part D implementation in 2006. The prevalence of spending less on basic needs was 10.6% in 2004, 11.1% in 2005, and 7.6% in 2006. Adjusted analyses comparing 2006 with 2005 and controlling for historical changes (2005 vs 2004) demonstrated significant decreases in the odds of CRN (ratio of odds ratios [ORs], 0.85; 95% confidence interval [CI], 0.74-0.98; P = .03) and spending less on basic needs (ratio of ORs, 0.59; 95% CI, 0.48-0.72; P < .001). No significant changes in CRN were observed among beneficiaries with fair to poor health (ratio of ORs, 1.00; 95% CI, 0.82-1.21; P = .97), despite high baseline CRN prevalence for this group (22.2% in 2005) and significant decreases among beneficiaries with good to excellent health (ratio of ORs, 0.77; 95% CI, 0.63-0.95; P = .02). However, significant reductions in spending less on basic needs were observed in both groups (fair to poor health: ratio of ORs, 0.60; 95% CI, 0.47-0.75; P < .001; and good to excellent health: ratio of ORs, 0.57; 95% CI, 0.44-0.75; P < .001).
Conclusions: In this survey population, there was evidence for a small but significant overall decrease in CRN and forgoing basic needs following Part D implementation. However, no net decrease in CRN after Part D was observed among the sickest beneficiaries, who continued to experience higher rates of CRN.
Figures
Comment in
-
Medicare Part D: a successful start with room for improvement.JAMA. 2008 Apr 23;299(16):1954-5. doi: 10.1001/jama.299.16.1954. JAMA. 2008. PMID: 18430916 Free PMC article. No abstract available.
-
Medication therapy management and cost-related medication nonadherence.JAMA. 2008 Sep 10;300(10):1130; author reply 1130-1. doi: 10.1001/jama.300.10.1130-a. JAMA. 2008. PMID: 18780839 No abstract available.
References
-
- Soumerai SB, Ross-Degnan D. Inadequate drug coverage in Medicare: A call to action. N Engl J Med. 1999;340:722–728. - PubMed
-
- Adams AS, Soumerai SB, Ross-Degnan D. The case for a Medicare drug coverage benefit: a critical review of the empirical evidence. Annual Review of Public Health. 2001;22:49–61. - PubMed
-
- Federman AD, Adams AS, Ross-Degnan D, Soumerai SB, Ayanian JZ. Supplemental insurance and use of effective cardiovascular drugs among elderly Medicare beneficiaries with coronary heart disease. JAMA. 2001;286:1732–1739. - PubMed
-
- Safran DG, Neuman P, Schoen C, Kitchman MS, Wilson I, Cooper B, Li A, Chang H, Rogers WH. Prescription drug coverage and seniors: where do things stand on the eve of implementing the new part d benefit? Findings from a 2003 National survey of seniors? Health Aff April. 2005;19:W5-152–W5-166. (web exclusive) - PubMed
-
- Soumerai SB, Pierre-Jacques M, Zhang F, Ross-Degnan D, Adams AS, Gurwitz J, Adler G, Safran DG. Cost-related medication nonadherence among the elderly and the disabled: A national survey one year before the Medicare drug benefit. Arch Intern Med. 2006;166:1829–1835. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
