

Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy
- PMID: 18433339
- PMCID: PMC2593910
- DOI: 10.1086/587667
Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy
Abstract
Background: Cryptococcal meningitis (CM) is the proximate cause of death in 20%-30% of persons with acquired immunodeficiency syndrome in Africa.
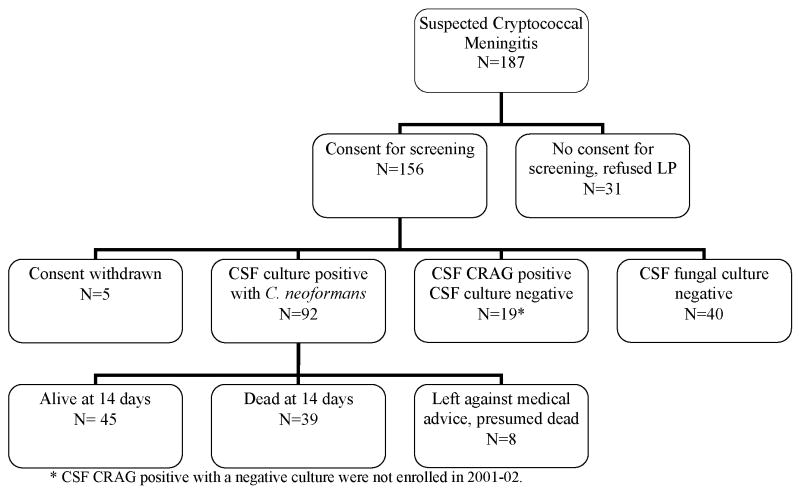
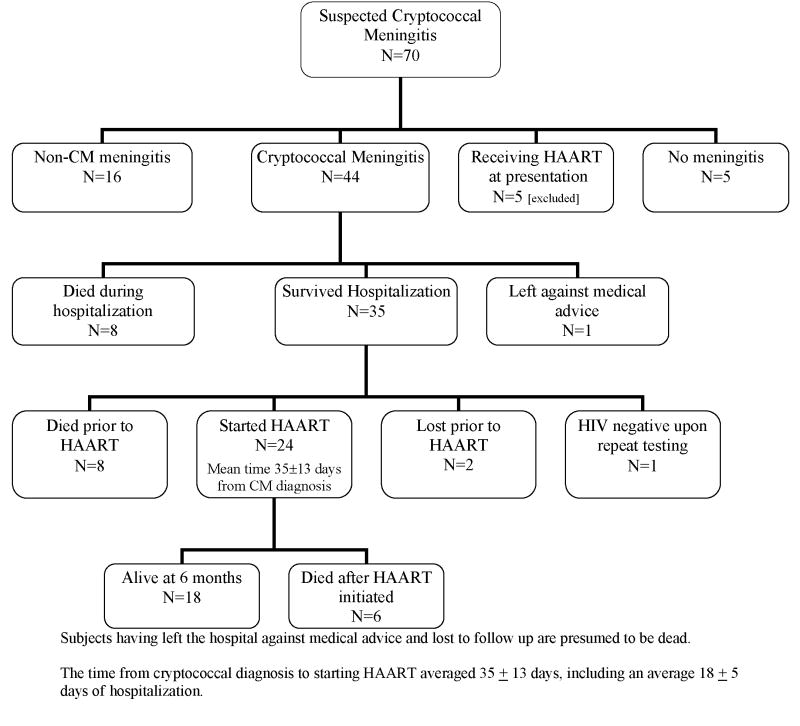
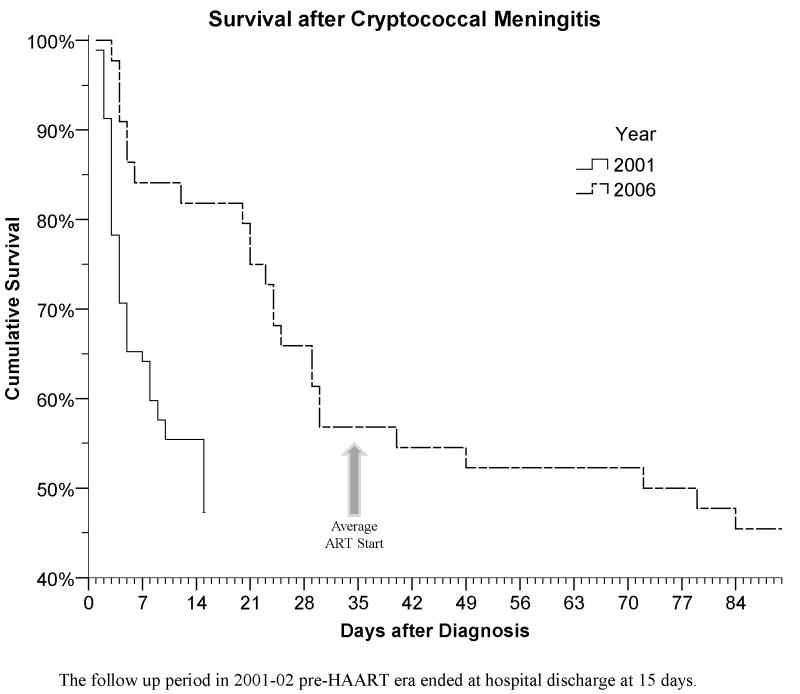
Methods: Two prospective, observational cohorts enrolled human immunodeficiency virus (HIV)-infected, antiretroviral-naive persons with CM in Kampala, Uganda. The first cohort was enrolled in 2001-2002 (n = 92), prior to the availability of highly active antiretroviral therapy (HAART), and the second was enrolled in 2006-2007 (n = 44), when HAART was available.
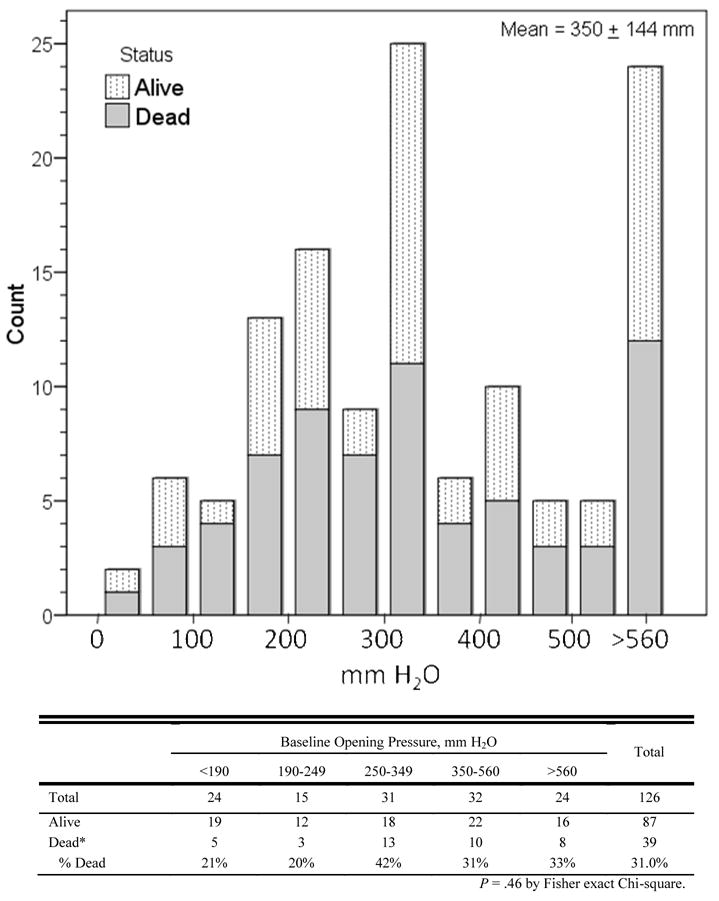
Results: Ugandans presented with prolonged CM symptoms (median duration, 14 days; interquartile range, 7-21 days). The 14-day survival rates were 49% in 2001-2002 and 80% in 2006 (P < .001). HAART was started 35 +/- 13 days after CM diagnosis and does not explain the improved 14-day survival rate in 2006. In 2006-2007, the survival rate continued to decrease after hospitalization, with only 55% surviving to initiate HAART as an outpatient. Probable cryptococcal-related immune reconstitution inflammatory syndrome occurred in 42% of patients, with 4 deaths. At 6 months after CM diagnosis, 18 persons (41%) were alive and receiving HAART in 2007. The median cerebral spinal fluid (CSF) opening pressure was 330 mm H(2)O; 81% of patients had elevated pressure (>200 mm H(2)O). Only 5 patients consented to therapeutic lumbar puncture. There was a trend for higher mortality for pressures >250 mm H(2)O (odds ratio [OR], 2.1; 95% confidence interval [CI], 0.9-5.2; P = .09). Initial CSF WBC counts of <5 cells/mL were associated with failure of CSF sterilization (OR, 17.3; 95% CI, 3.1-94.3; P < .001), and protein levels <35 mg/dL were associated with higher mortality (OR, 2.0; 95% CI, 1.2-3.3; P = .007).
Conclusions: Significant CM-associated mortality persists, despite the administration of amphotericin B and HIV therapy, because of the high mortality rate before receipt of HAART and because of immune reconstitution inflammatory syndrome-related complications after HAART initiation. Approaches to increase acceptance of therapeutic lumbar punctures are needed.
Conflict of interest statement
Conflicts of Interest: No conflicts of interest exist.
Figures
References
-
- Hakim JG, Gangaidzo IT, Heyderman RS, et al. Impact of HIV infection on meningitis in Harare, Zimbabwe: a prospective study of 406 predominantly adult patients. AIDS. 2000;14:1401–7. - PubMed
-
-
“3 by 5” Progress Report: December 2003-June 2004, July 2004 WHO Publication
-
-
- Chuck SL, Sande MA. Infection with Cryptococcus neoformans in the Acquired Immunodeficiency Syndrome. N Engl J Med. 1989;231:794–9. - PubMed
-
- French N, Gray K, Watera C, et al. Cryptococcal infection in a cohort of HIV-1-infected Ugandan adults. AIDS. 2002;16:1031–8. - PubMed
-
- Sacktor N, Lyles RH, Skolasky MA, et al. HIV-associated neurologic diseases incidence changes: Multicenter AIDS cohort Study, 1990–1998. Neurology. 2001;56:257–260. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
