

Eosinopenia is a reliable marker of sepsis on admission to medical intensive care units
- PMID: 18435836
- PMCID: PMC2447615
- DOI: 10.1186/cc6883
Eosinopenia is a reliable marker of sepsis on admission to medical intensive care units
Abstract
Introduction: Eosinopenia is a cheap and forgotten marker of acute infection that has not been evaluated previously in intensive care units (ICUs). The aim of the present study was to test the value of eosinopenia in the diagnosis of sepsis in patients admitted to ICUs.
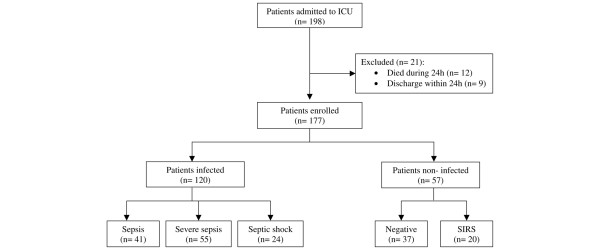
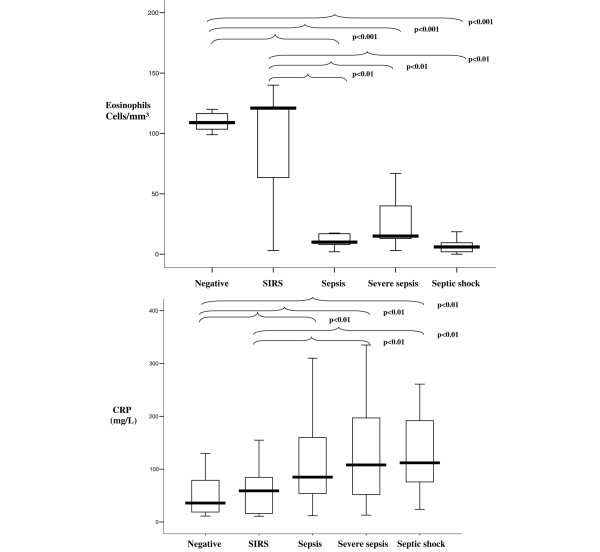
Methods: A prospective study of consecutive adult patients admitted to a 12-bed medical ICU was performed. Eosinophils were measured at ICU admission. Two intensivists blinded to the eosinophils classified patients as negative or with systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, or septic shock.
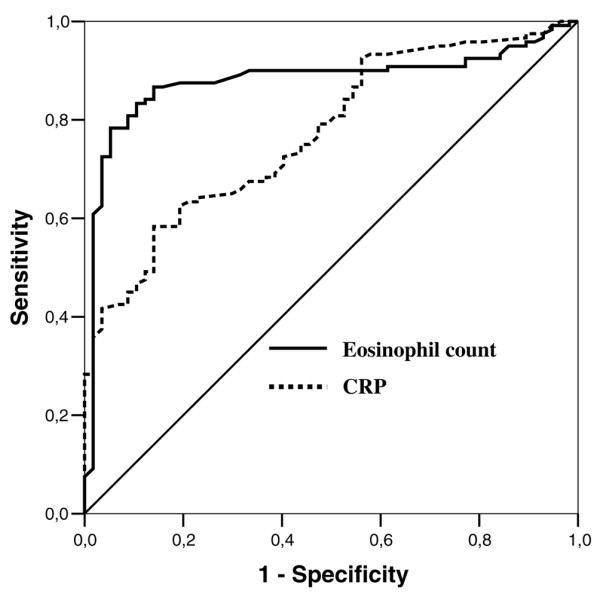
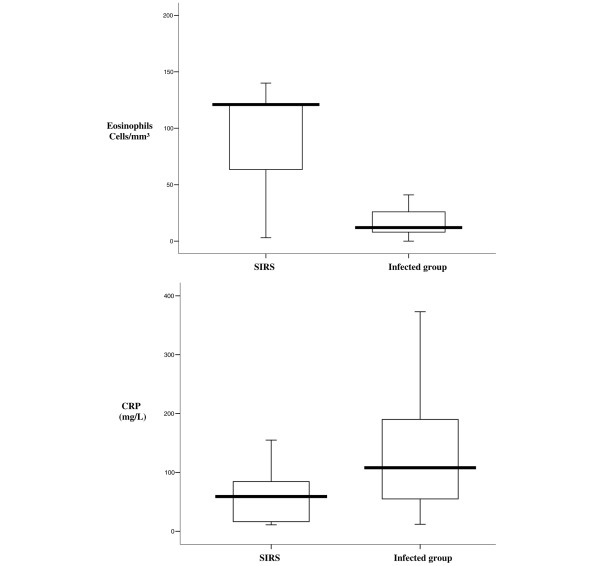
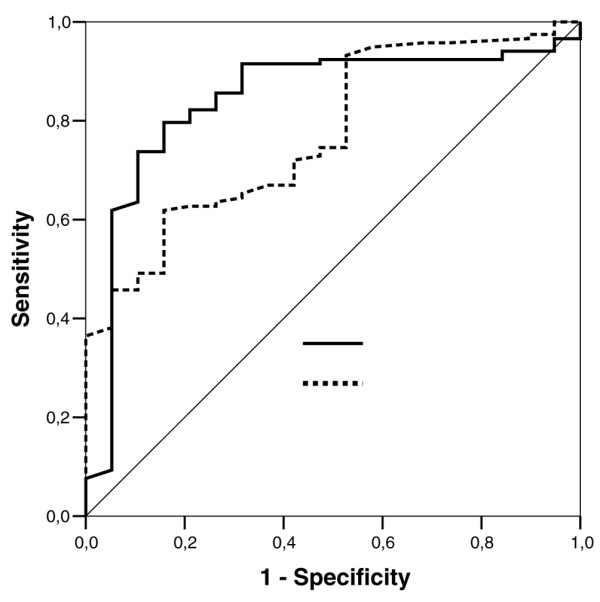
Results: A total of 177 patients were enrolled. In discriminating noninfected (negative + SIRS) and infected (sepsis + severe sepsis + septic shock) groups, the area under the receiver operating characteristic curve was 0.89 (95% confidence interval (CI), 0.83 to 0.94). Eosinophils at <50 cells/mm3 yielded a sensitivity of 80% (95% CI, 71% to 86%), a specificity of 91% (95% CI, 79% to 96%), a positive likelihood ratio of 9.12 (95% CI, 3.9 to 21), and a negative likelihood ratio of 0.21(95% CI, 0.15 to 0.31). In discriminating SIRS and infected groups, the area under the receiver operating characteristic curve was 0.84 (95% CI, 0.74 to 0.94). Eosinophils at <40 cells/mm3 yielded a sensitivity of 80% (95% CI, 71% to 86%), a specificity of 80% (95% CI, 55% to 93%), a positive likelihood ratio of 4 (95% CI, 1.65 to 9.65), and a negative likelihood ratio of 0.25 (95% CI, 0.17 to 0.36).
Conclusion: Eosinopenia is a good diagnostic marker in distinguishing between noninfection and infection, but is a moderate marker in discriminating between SIRS and infection in newly admitted critically ill patients. Eosinopenia may become a helpful clinical tool in ICU practices.
Figures
Comment in
-
Role of the eosinophil count in discriminating the severity of community-acquired pneumonia in HIV-infected patients.Crit Care. 2008;12(4):425; author reply 425. doi: 10.1186/cc6971. Epub 2008 Aug 13. Crit Care. 2008. PMID: 18710601 Free PMC article. No abstract available.
-
Is eosinopenia a reliable marker of sepsis?Crit Care. 2009;13(3):409. doi: 10.1186/cc7877. Epub 2009 Jun 1. Crit Care. 2009. PMID: 19519944 Free PMC article. No abstract available.
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definition for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101:1644–1655. doi: 10.1378/chest.101.6.1644. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
