

Umbilical port-site complications in laparoscopic cholecystectomy: role of topical antibiotic therapy
- PMID: 18435883
- PMCID: PMC3016169
Umbilical port-site complications in laparoscopic cholecystectomy: role of topical antibiotic therapy
Abstract
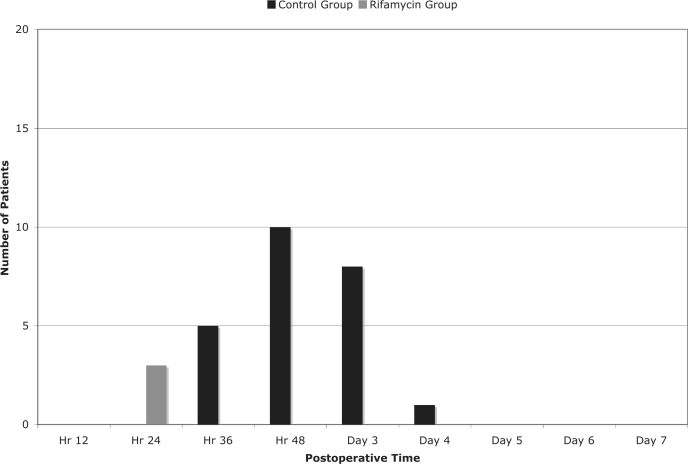
Background and objectives: Umbilical port-site infections after video-laparoscopic cholecystectomy (VLC) are frequent complications. The aim of this prospective randomized study was to verify the validity of topical rifamycin for prevention of post-VLC umbilical infections.
Methods: From September 2006 to April 2007, 48 patients with uncomplicated cholelithiasis who underwent VLC were enrolled in the study. Enrolled patients were randomized into 2 groups. The first group of 24 patients was treated with topical rifamycin to the umbilicus. The second group of 24 patients was not treated with rifamycin.
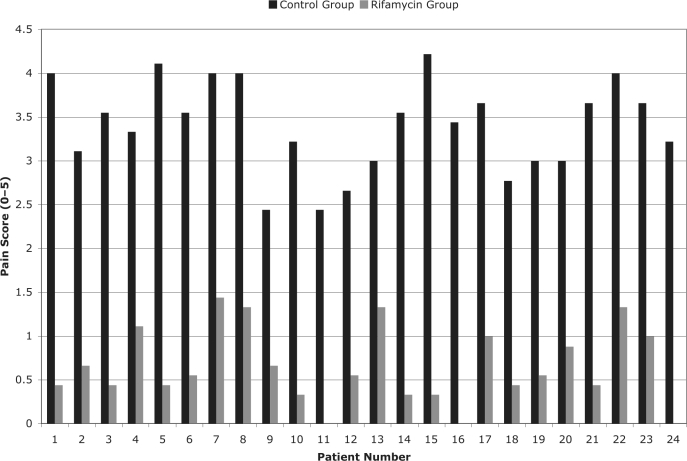
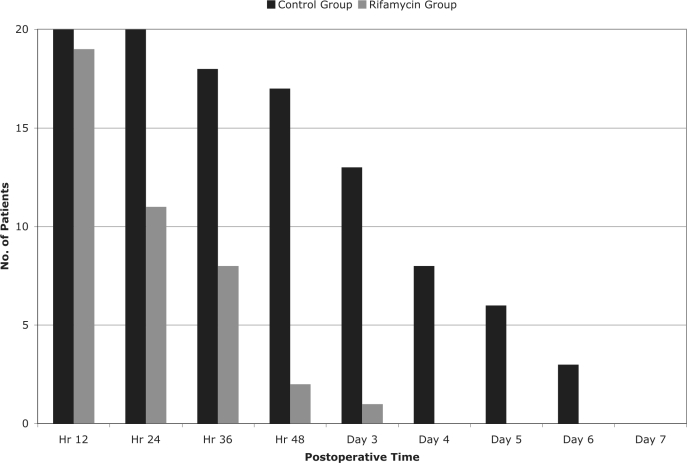
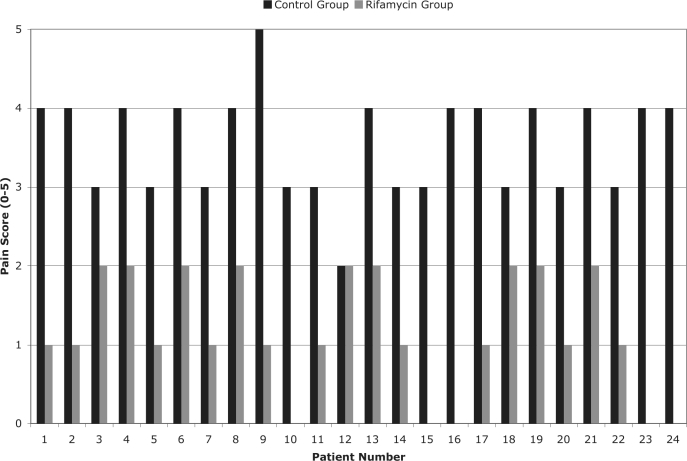
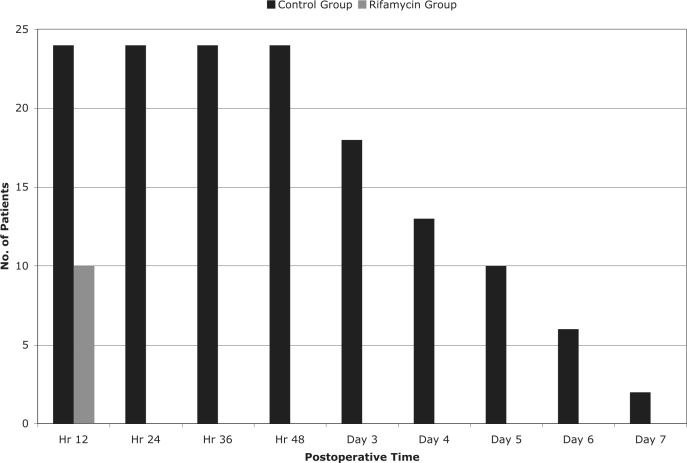
Results: Postoperative umbilical pain with a need for analgesics, presence of signs of inflammation of the umbilical wound, dehiscence of the umbilical skin sutures, and the presence of incisional umbilical hernia on the 60th postoperative day were statistically significantly better in the rifamycin group compared with the control group.
Conclusions: Topical administration of rifamycin to the umbilicus in the pre-, intra- and postoperative periods was a rapid, safe, and economic way to reduce infective complications after VLC.
Figures
References
-
- Hamzaoglu I, Baca HB, Boler DE, Polat E, Ozer Y. Is umbilical flora responsible for wound infection after laparoscopic surgery? Surg Laparosc Endosc Percutan Tech 2004;14(5):263–267 - PubMed
-
- Voitk AJ, Tsao SGS. The umbilicus in laparoscopic Surgery. Surg Endosc. 2001;15(8):878–881 - PubMed
-
- Molloy D, Kaloo PD, Cooper M, Nguyen TV. Laparoscopic entry: a literature review and analysis of techniques and complications of primary port entry. Aust N Z J Obstet Gynaecol. 2002;42(3):246. - PubMed
-
- Australian Safety and Efficacy Register of New Interventional Procedures–Surgical. Consumer Summary: Methods Used to Establish Laparoscopic Pneumoperitoneum (Adapted from the Report of the Review Group for Consumer Use by Ms. E. Ahern) Melbourne Australia: Royal Australian College of Surgeons; March 2002
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous