

Predictive power of sequential measures of albuminuria for progression to ESRD or death in Pima Indians with type 2 diabetes
- PMID: 18436086
- PMCID: PMC2386511
- DOI: 10.1053/j.ajkd.2008.01.011
Predictive power of sequential measures of albuminuria for progression to ESRD or death in Pima Indians with type 2 diabetes
Abstract
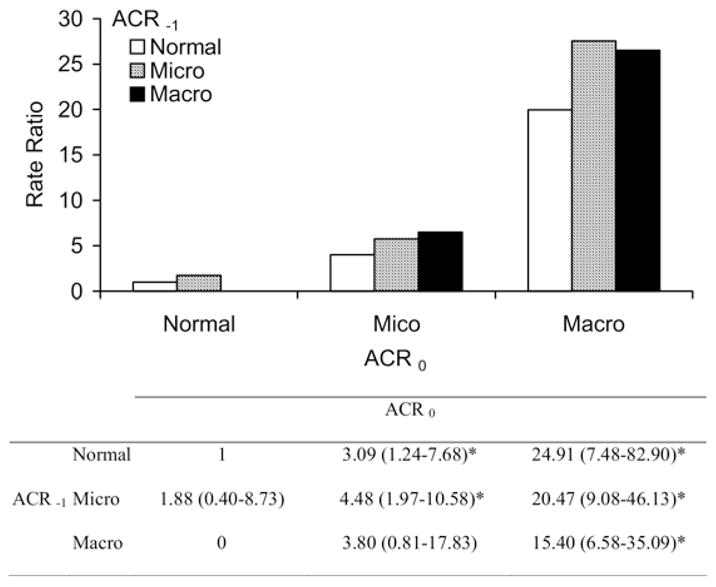
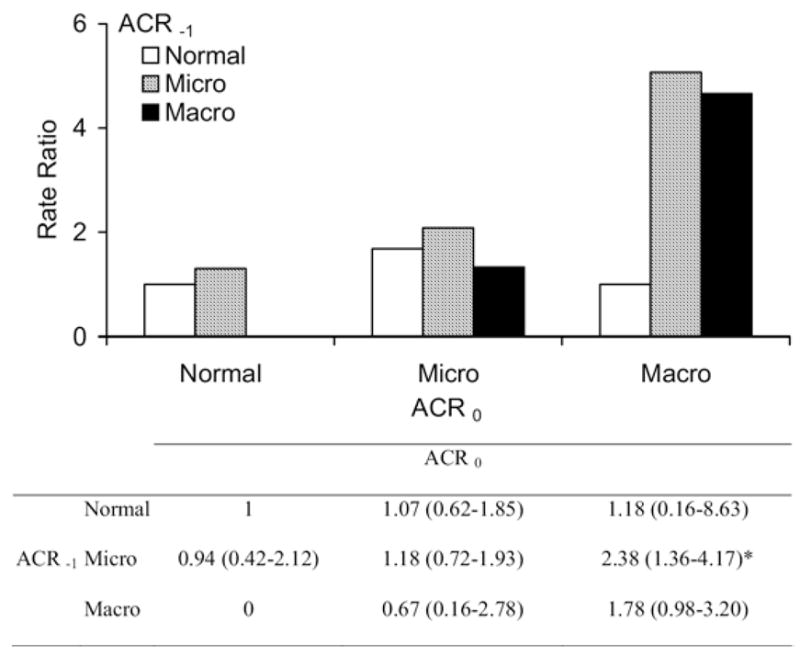
Background: To determine whether historic albuminuria measurements provide additional predictive value for diabetic end-stage renal disease (ESRD) and natural mortality over the most recent measurement, ie, whether "regression" from high albuminuria has a different prognosis than stability at the lower level.
Study design: Observational longitudinal study.
Setting & participants: Pima Indians 15 years or older with type 2 diabetes and at least 2 consecutive measurements of urinary albumin-creatinine ratio (ACR) within 6 years.
Predictors: Sequential measurements of urinary ACR.
Outcomes & measurements: Proportional hazards analyses were used to estimate the risk of ESRD and natural death associated with the first and second ACR measurement. The ability of these highly correlated variables to predict outcome was compared with receiver operating characteristic curves calculated by means of the generalized c statistic.
Results: In 983 subjects, 136 developed ESRD and 180 died of natural causes during a maximum follow-up of 12.6 years. Each doubling in the second ACR was associated with a 1.71-fold greater incidence of ESRD (95% confidence interval, 1.54 to 1.89) and 1.16-fold greater natural mortality (95% confidence interval, 1.07 to 1.27) adjusted for age, sex, diabetes duration, and antihypertensive medication. The addition of the first ACR measurement to the model did not add to the predictive value for ESRD or mortality. In pairwise comparisons of c statistics, the second ACR was a significantly better predictor of ESRD than the first ACR.
Limitations: The predictive value of ACR measurements is decreased to the extent that its precision is based on a single measure.
Conclusion: The predictive power of the latest ACR for ESRD and natural mortality in patients with diabetes is not enhanced by knowledge of the preceding ACR. Therefore, ACR changes over time, ie, regression or progression, add minimal predictive value beyond the latest measurement in the series.
Figures
References
-
- Perkins BA, Ficociello LH, Silva KH, Finkelstein DM, Warram JH, Krolewski AS. Regression of microalbuminuria in type 1 diabetes. N Engl J Med. 2003;348:2285–2293. - PubMed
-
- Araki S, Haneda M, Sugimoto T, et al. Factors associated with frequent remission of microalbuminuria in patients with type 2 diabetes. Diabetes. 2005;54:2983–2987. - PubMed
-
- Spoelstra-de Man AME, Brouwer CB, Stehouwer CDA, Smulders YM. Rapid progression of albumin excretion is an independent predictor of cardiovascular mortality in patients with type 2 diabetes and microalbuminuria. Diabetes Care. 2001;24:2097–2101. - PubMed
-
- Gaede P, Tarnow L, Vedel P, Parving HH, Pedersen O. Remission to normoalbuminuria during multifactorial treatment preserves kidney function in patients with type 2 diabetes and microalbuminuria. Nephrol Dial Transplant. 2004;19:2784–2788. - PubMed
-
- Rossing K, Christensen PK, Hovind P, Parving HH. Remission of nephrotic-range albuminuria reduces risk of end-stage renal disease and improves survival in type 2 diabetic patients. Diabetologia. 2005;48:2241–2247. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
