

Radiofrequency ablation with the real-time virtual sonography system for treating hepatocellular carcinoma difficult to detect by ultrasonography
- PMID: 18437215
- PMCID: PMC2291506
- DOI: 10.3164/jcbn.40.66
Radiofrequency ablation with the real-time virtual sonography system for treating hepatocellular carcinoma difficult to detect by ultrasonography
Abstract
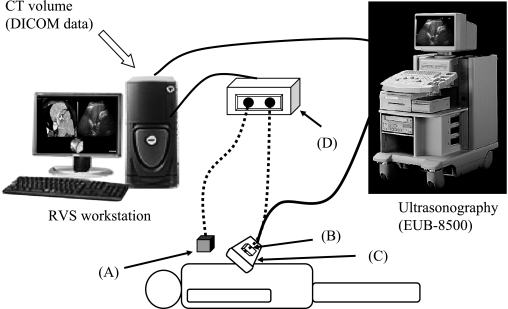
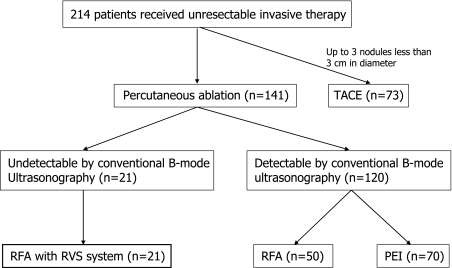
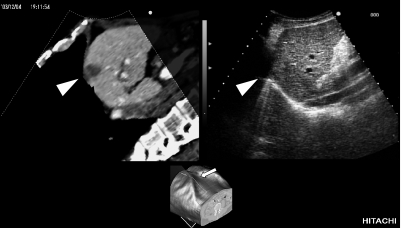
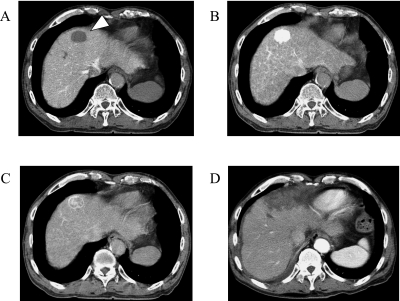
Radiofrequency ablation has been applied to treat hepatocellular carcinoma, with favorable therapeutic outcomes. Nevertheless, practitioners have approached radiofrequency ablation with some reluctance due to the difficulty of identifying isoechoic tumors and recurrent tumors. The aim of the present study is to investigate the efficacy of Real-time Virtual Sonography to treat hepatocellular carcinoma difficult to detect by conventional ultrasonography. Real-time Virtual Sonography is a system generating multiplanar reconstruction images in real-time using the Hitachi medico EUB-8500 equipped with a probe. The system included following components: 1) digital imaging and communications in medicine (DICOM) data from dynamic CT, 2) a magnetic field generator to match the multiplanar reconstruction image on the monitor and the actual ultrasonography image, 3) the cross section with the tumor displayed as a multiplanar reconstruction image. Total twenty-five nodules of twenty-one patients underwent radiofrequency ablation monitored by Real-time Virtual Sonography. All nodules difficult to detect via conventional ultrasonography were clearly visualized in real-time. The average nodule diameter was 2.4 +/- 1.6 cm, and punctures and coagulation were performed an average of 2.2 and 3 times per session. Dynamic CT after session confirmed effective coagulation of each nodule. In conclusion, this study demonstrates that the present system is capable of effectively and accurately treating tumors difficult to detect by conventional ultrasonography.
Keywords: HCV; coagulation; dynamic CT; hepatic tumor; multiplanar reconstruction image.
Figures
References
-
- Bruix J., Sherman M., Llovet J.M., Beaugrand M., Lencioni R., Burroughs A.K., Christensen E., Pagliaro L., Colombo M., Rodes J. EASL Panel of Experts on HCC.: Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J. Hepatol. 2001;35:421–430. - PubMed
-
- Bruix J., Llovet J.M. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 2002;35:519–524. - PubMed
-
- Lam C.M., Ng K.K., Poon R.T., Ai V., Yuen J., Fan S.T. Impact of radiofrequency ablation on the management of patients with hepatocellular carcinoma in a specialized centre. Br. J. Surg. 2004;91:334–338. - PubMed
-
- Matsui O., Takashima T., Kadoya M., Ida M., Suzuki M., Kitagawa K., Kamimura R., Inoue K., Konishi H., Itoh H. Dynamic computed tomography during arterial portography: the most sensitive examination for small hepatocellular carcinoma. J. Comput. Assist. Tomogr. 1985;9:19–24. - PubMed