

Progress and prospects in male hormonal contraception
- PMID: 18438174
- PMCID: PMC2664382
- DOI: 10.1097/MED.0b013e3282fcc30d
Progress and prospects in male hormonal contraception
Abstract
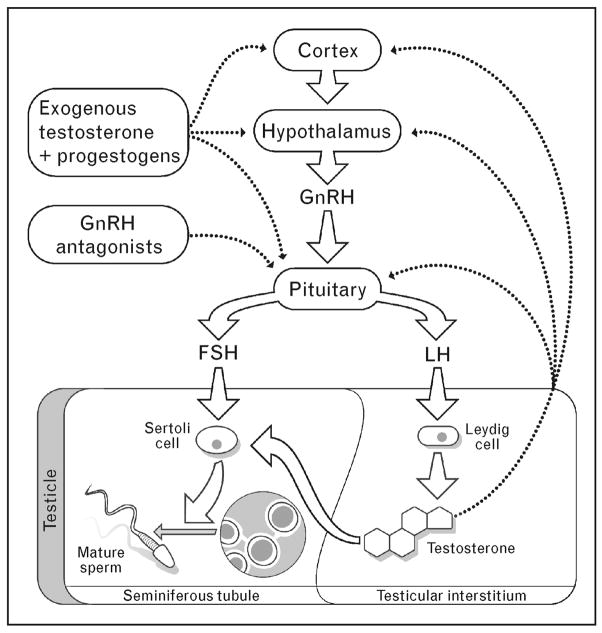
Purpose of review: Testosterone functions as a contraceptive by suppressing the secretion of luteinizing hormone and follicle-stimulating hormone from the pituitary. Low concentrations of these hormones deprive the testes of the signals required for spermatogenesis and results in markedly decreased sperm concentrations and effective contraception in a majority of men. Male hormonal contraception is well tolerated and acceptable to most men. Unfortunately, testosterone-alone regimens fail to completely suppress spermatogenesis in all men, meaning that in some the potential for fertility remains.
Recent findings: Because of this, novel combinations of testosterone and progestins, which synergistically suppress gonadotropins, have been studied. Two recently published testosterone/progestin trials are particularly noteworthy. In the first, a long-acting injectable testosterone ester, testosterone decanoate, was combined with etonogestrel implants and resulted in 80-90% of subjects achieving a fewer than 1 million sperm per milliliter. In the second, a daily testosterone gel was combined with 3-monthly injections of depot medroxyprogesterone acetate producing similar results.
Summary: Testosterone-based hormone combinations are able to reversibly suppress human spermatogenesis; however, a uniformly effective regimen has remained elusive. Nevertheless, improvements, such as the use of injectable testosterone undecanoate, may lead to a safe, reversible and effective male contraceptive.
Figures
References
-
- Martin CW, Anderson RA, Cheng L, et al. Potential impact of hormonal male contraception: cross-cultural implications for development of novel male preparations. Hum Reprod. 2000;15:637–645. - PubMed
-
- Heinemann K, Saad F, Wiesemes M, et al. Attitudes toward male fertility control: results of a multinational survey on four continents. Hum Reprod. 2005;20:549–556. - PubMed
-
- Glasier AF, Anakwe R, Everington D, et al. Would women trust their partners to use a male pill? Hum Reprod. 2000;15:646–649. - PubMed
-
- Liu PY, Swerdloff RS, Christenson PD, et al. Hormonal Male Contraception Summit Group. Rate, extent, and modifiers of spermatogenic recovery after hormonal male contraception: an integrated analysis. Lancet. 2006;367:1412–1420. - PubMed
-
- World Health Organization Task Force on Methods for the Regulation of Male Fertility. Contraceptive efficacy of testosterone-induced azoospermia and oligozoospermia in normal men. Fertil Steril. 1996;65:821–829. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
