

Resuscitating the microcirculation in sepsis: the central role of nitric oxide, emerging concepts for novel therapies, and challenges for clinical trials
- PMID: 18439194
- PMCID: PMC2727641
- DOI: 10.1111/j.1553-2712.2008.00109.x
Resuscitating the microcirculation in sepsis: the central role of nitric oxide, emerging concepts for novel therapies, and challenges for clinical trials
Abstract
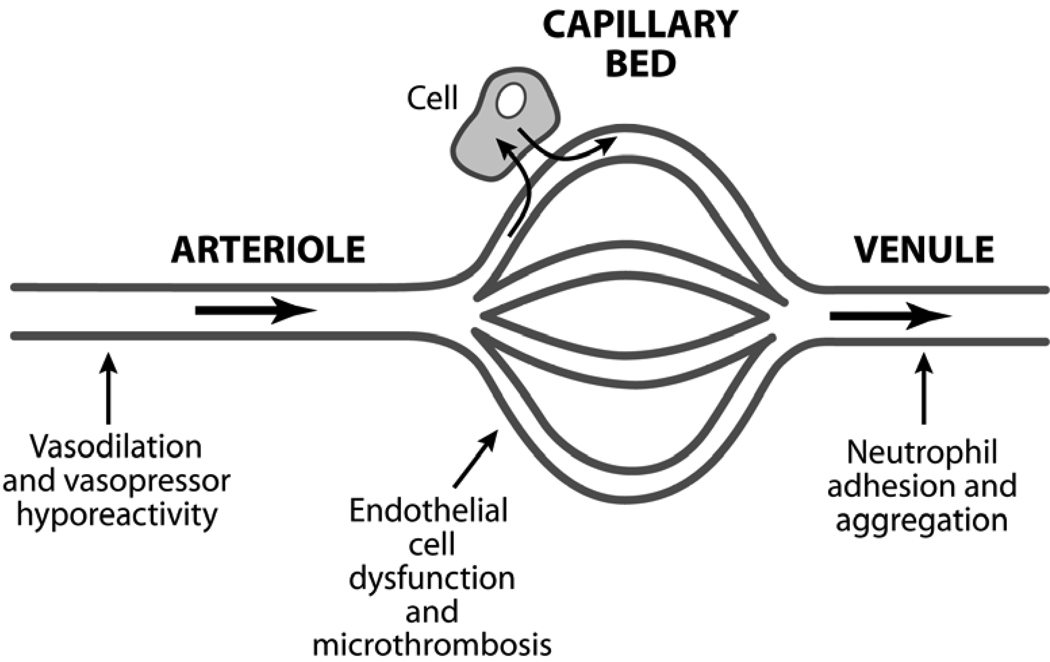
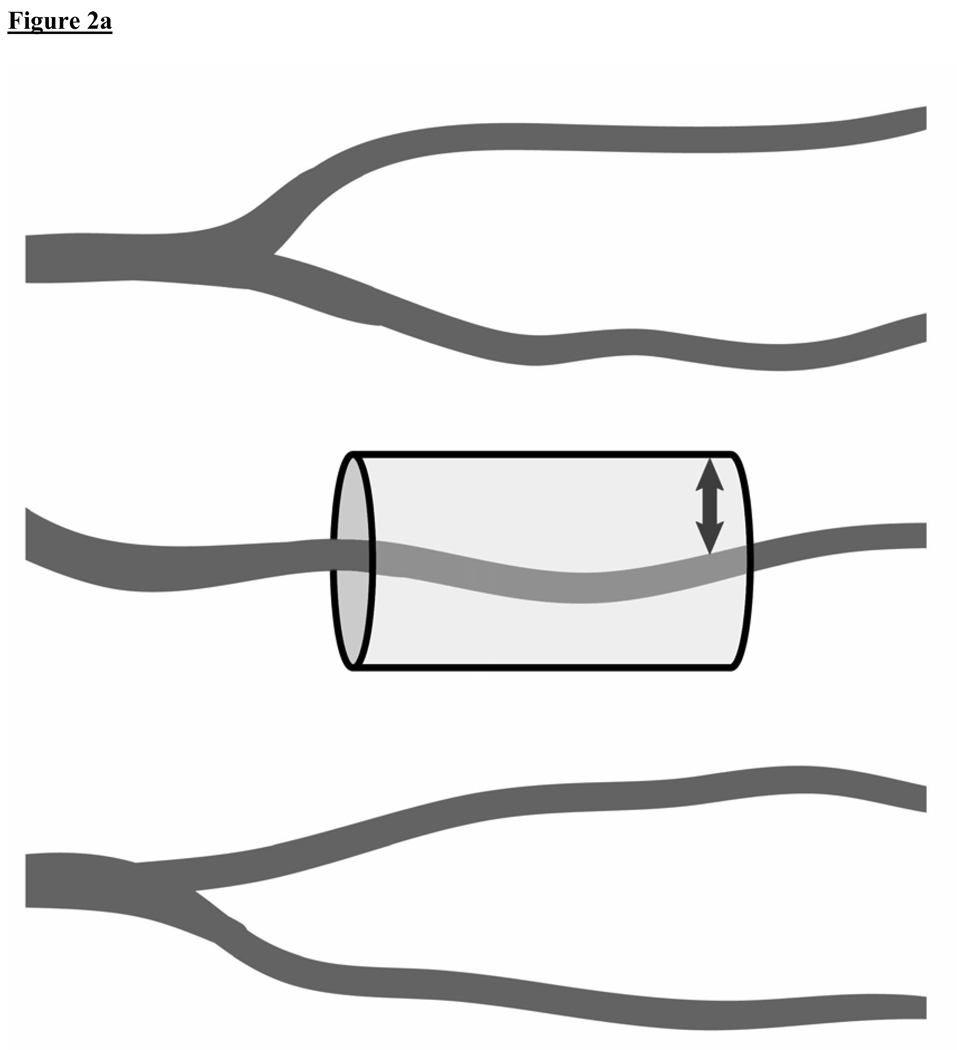
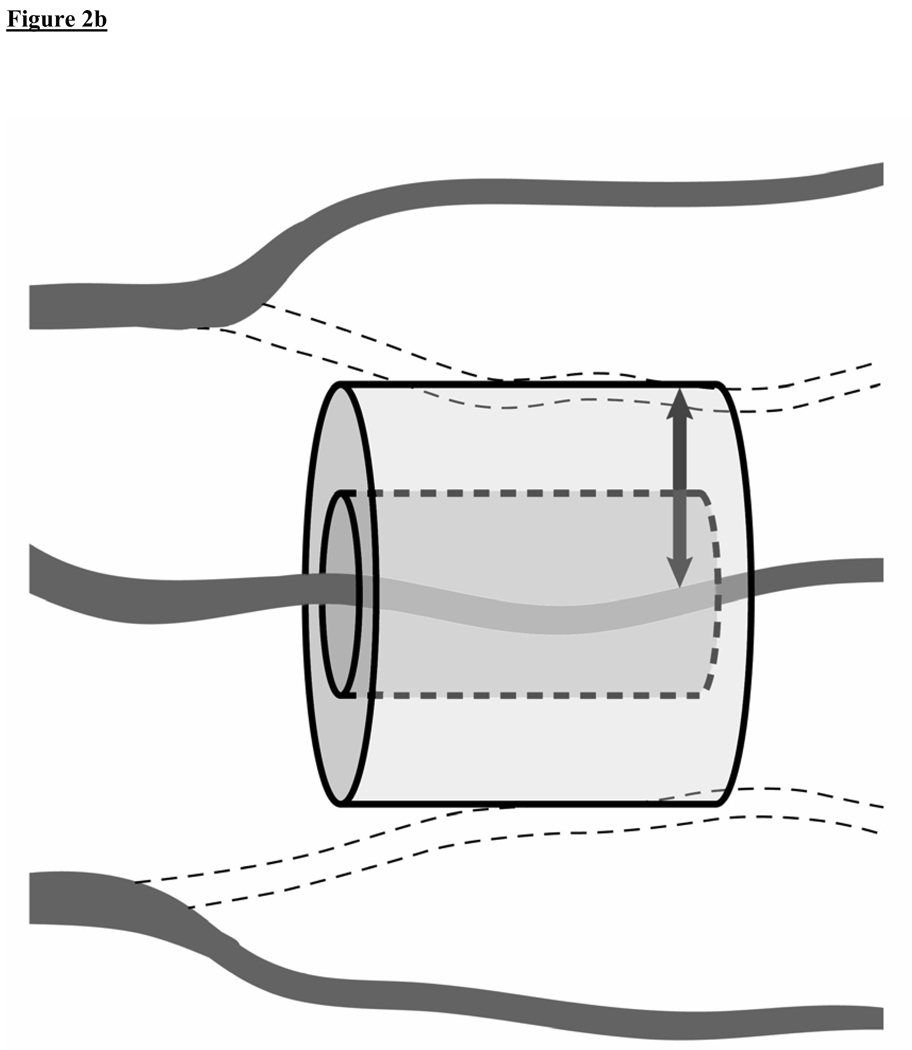
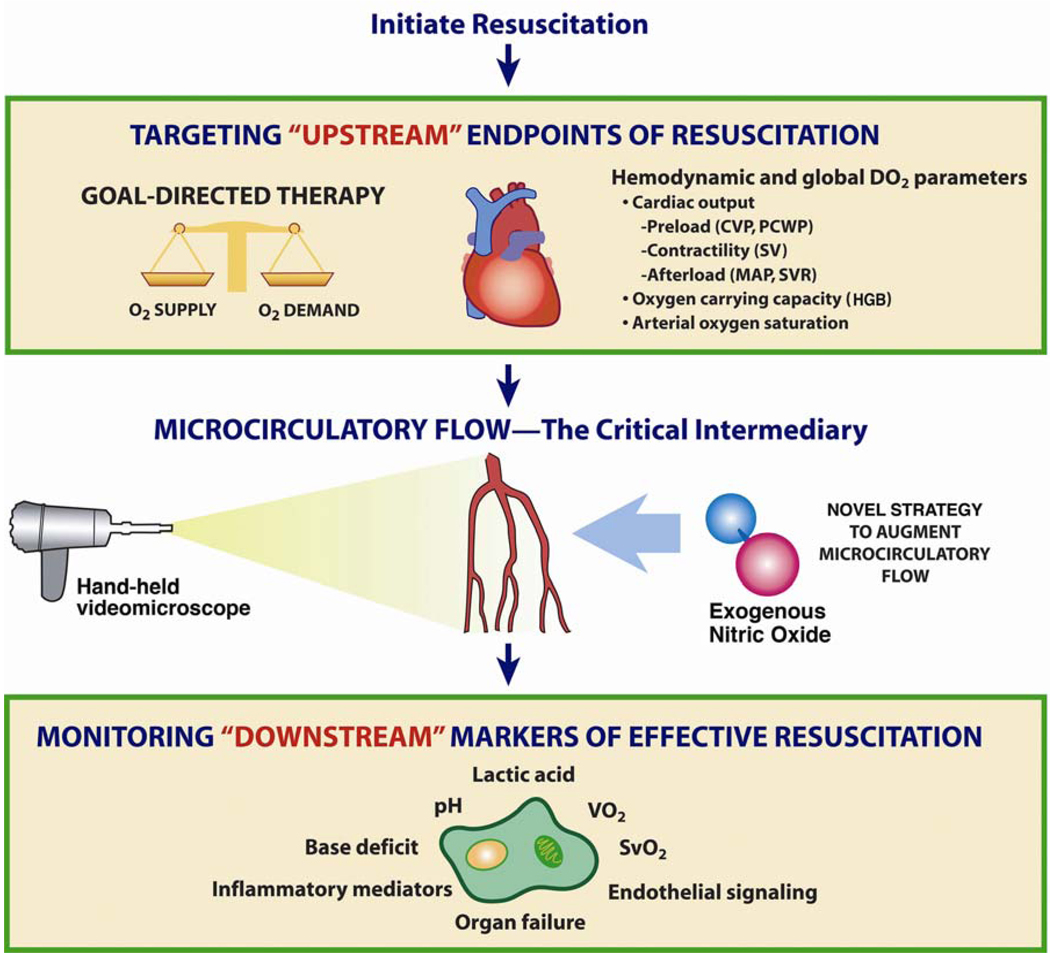
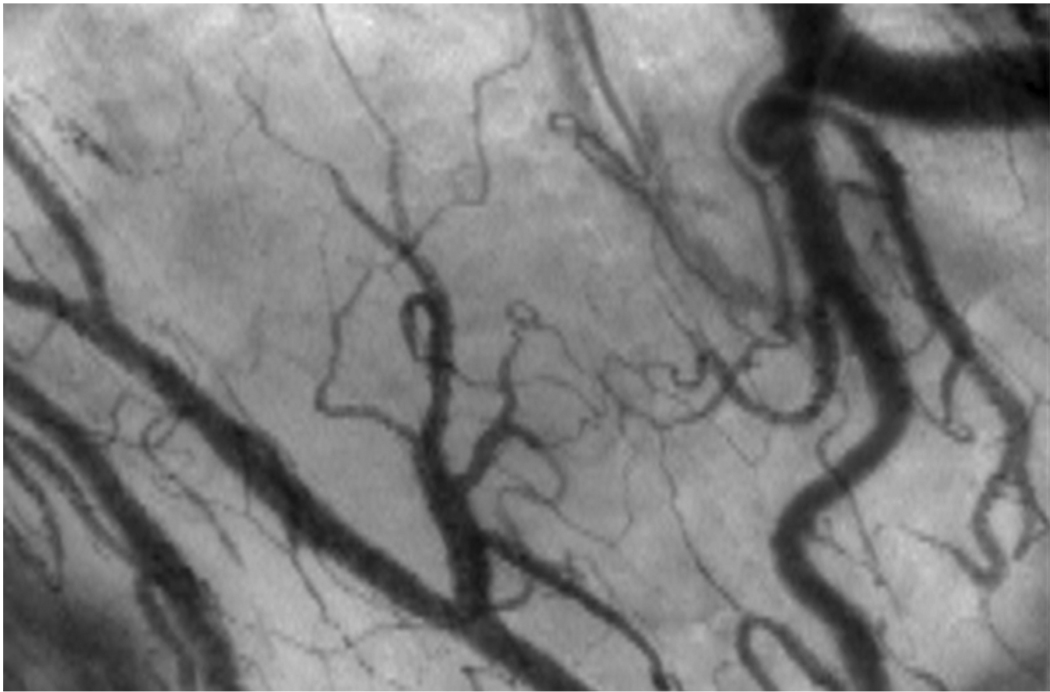
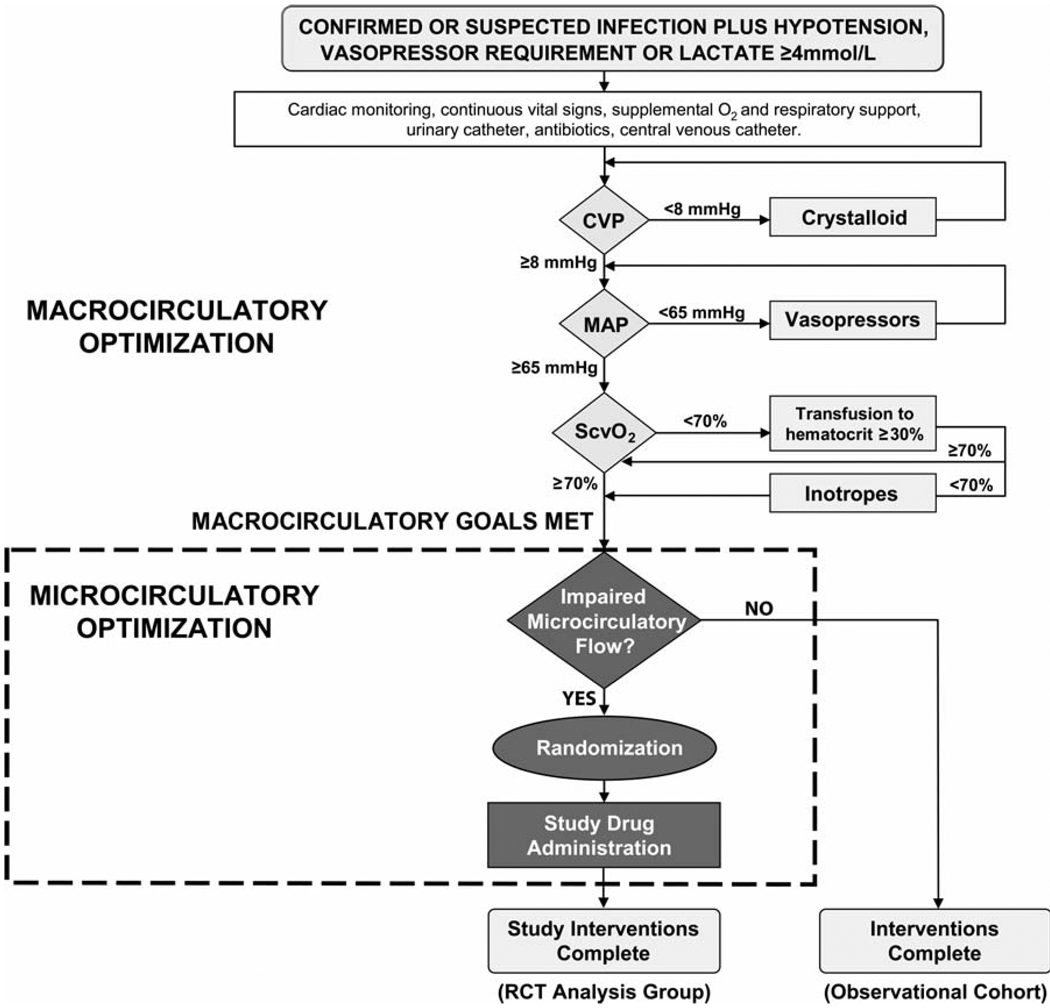
Microcirculatory dysfunction is a critical element of the pathogenesis of severe sepsis and septic shock. In this Bench-to-Bedside review, we present: 1) the central role of the microcirculation in the pathophysiology of sepsis; 2) new translational research techniques of in vivo video microscopy for assessment of microcirculatory flow in human subjects; 3) clinical investigations that reported associations between microcirculatory dysfunction and outcome in septic patients; 4) the potential role of novel agents to "rescue" the microcirculation in sepsis; 5) current challenges facing this emerging field of clinical investigation; and 6) a framework for the design of future clinical trials aimed to determine the impact of novel agents on microcirculatory flow and organ failure in patients with sepsis. We specifically focus this review on the central role and vital importance of the nitric oxide (NO) molecule in maintaining microcirculatory homeostasis and patency, especially when the microcirculation sustains an insult (as with sepsis). We also present the scientific rationale for clinical trials of exogenous NO administration to treat microcirculatory dysfunction and augment microcirculatory blood flow in early sepsis therapy.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001 Jul;29(7):1303–1310. - PubMed
-
- Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med. 2003 Jan 9;348(2):138–150. - PubMed
-
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006 Jun;34(6):1589–1596. - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19):1368–1377. - PubMed
-
- Lin SM, Huang CD, Lin HC, Liu CY, Wang CH, Kuo HP. A modified goal-directed protocol improves clinical outcomes in intensive care unit patients with septic shock: a randomized controlled trial. Shock. 2006 Dec;26(6):551–557. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
