

Hepatic involvement and portal hypertension predict mortality in chronic granulomatous disease
- PMID: 18439425
- PMCID: PMC2583937
- DOI: 10.1053/j.gastro.2008.02.081
Hepatic involvement and portal hypertension predict mortality in chronic granulomatous disease
Abstract
Background & aims: Chronic granulomatous disease (CGD) is a rare genetic disorder, predisposing affected individuals to recurrent infectious complications and shortened survival. Liver involvement in CGD includes vascular abnormalities, which may lead to noncirrhotic portal hypertension.
Methods: To evaluate the impact of noncirrhotic portal hypertension on survival in CGD, all records from 194 patients followed up at the National Institutes of Health with CGD were reviewed. Cox proportional hazards regression was used to determine factors associated with mortality.
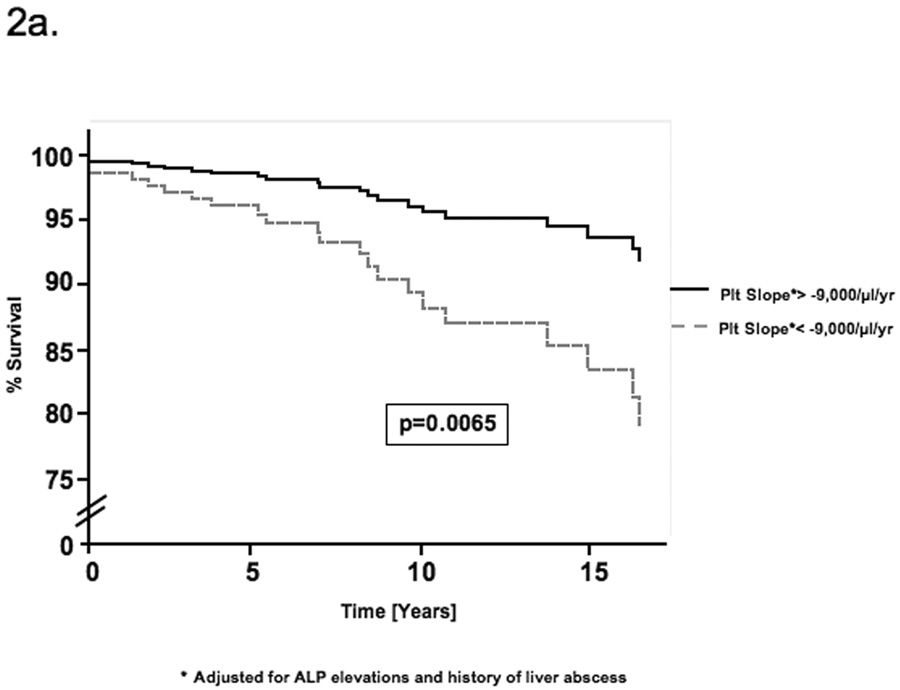
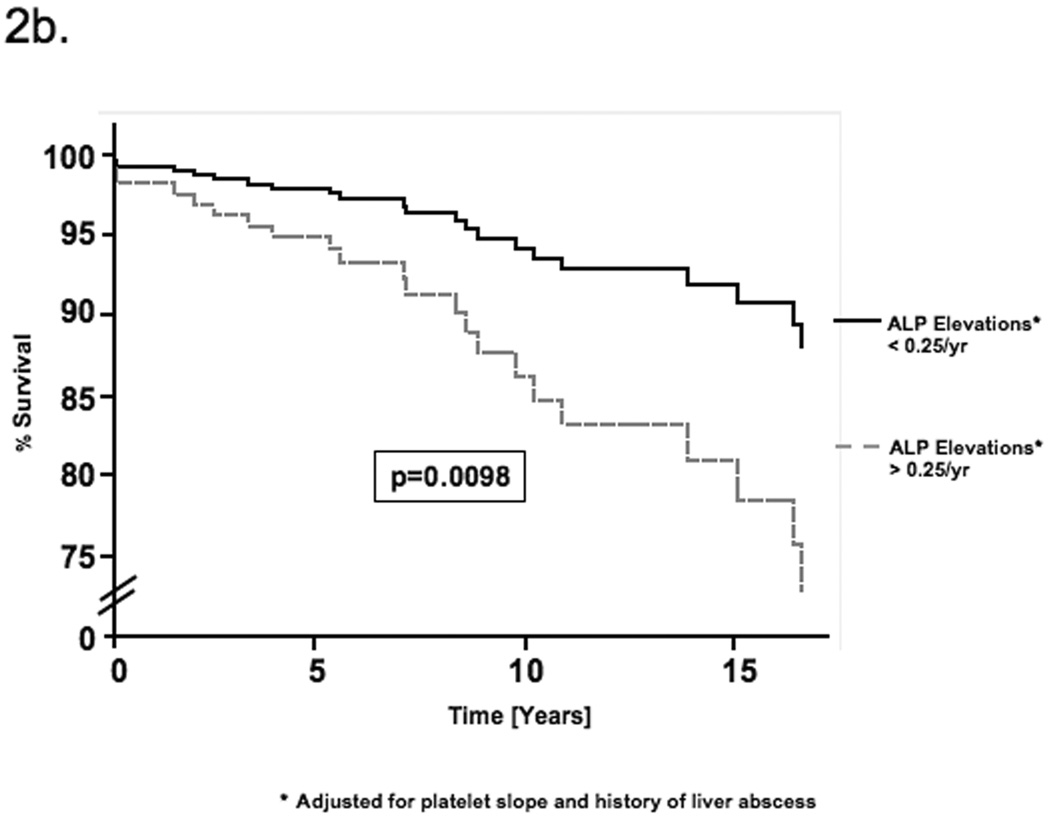
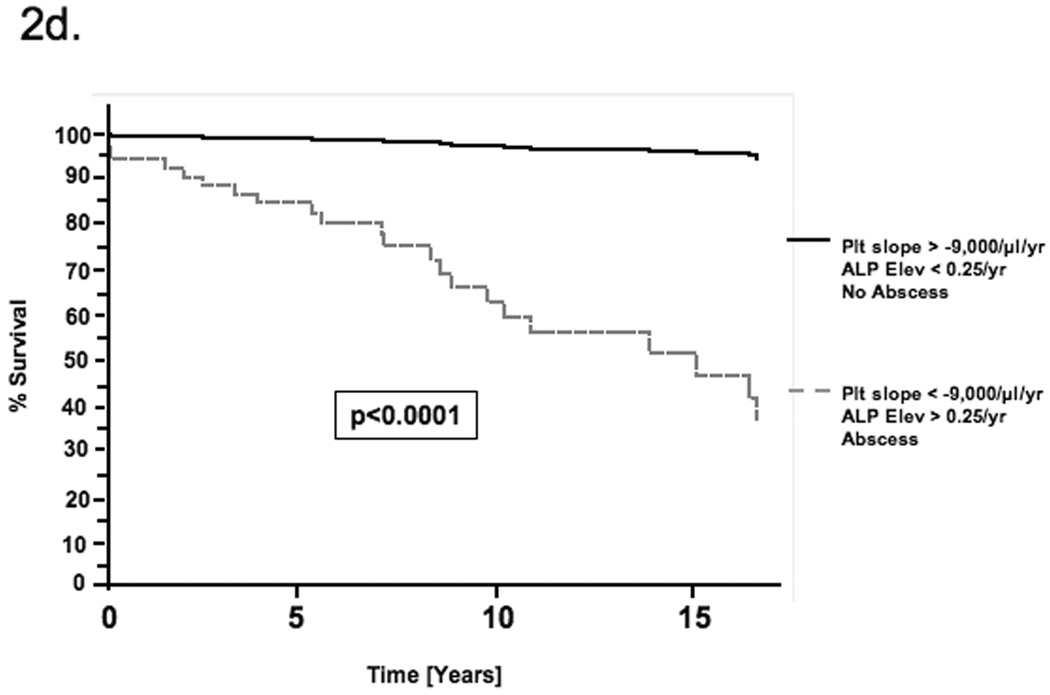
Results: Twenty-four patients died, all from infectious complications. By Cox regression, factors associated with mortality were as follows: (1) decreases in platelet count (>9000/microL/y; hazard ratio, 4.7; P = .007), (2) alkaline phosphatase level increases (>0.25/y; hazard ratio, 4.5; P = .01) and (3) history of liver abscess (hazard ratio, 3.1; P = .03). By regression analysis, decreasing platelet count was associated with increasing portal vein diameter, splenomegaly, increased serum immunoglobulin G level, and increasing number of alanine aminotransferase increases; greater number of alkaline phosphatase level increases and abscess were both associated with increasing age and number of infections. Prospective evaluation revealed increased hepatic-venous pressure gradients in 2 patients with progressive thrombocytopenia, suggestive of portal hypertension.
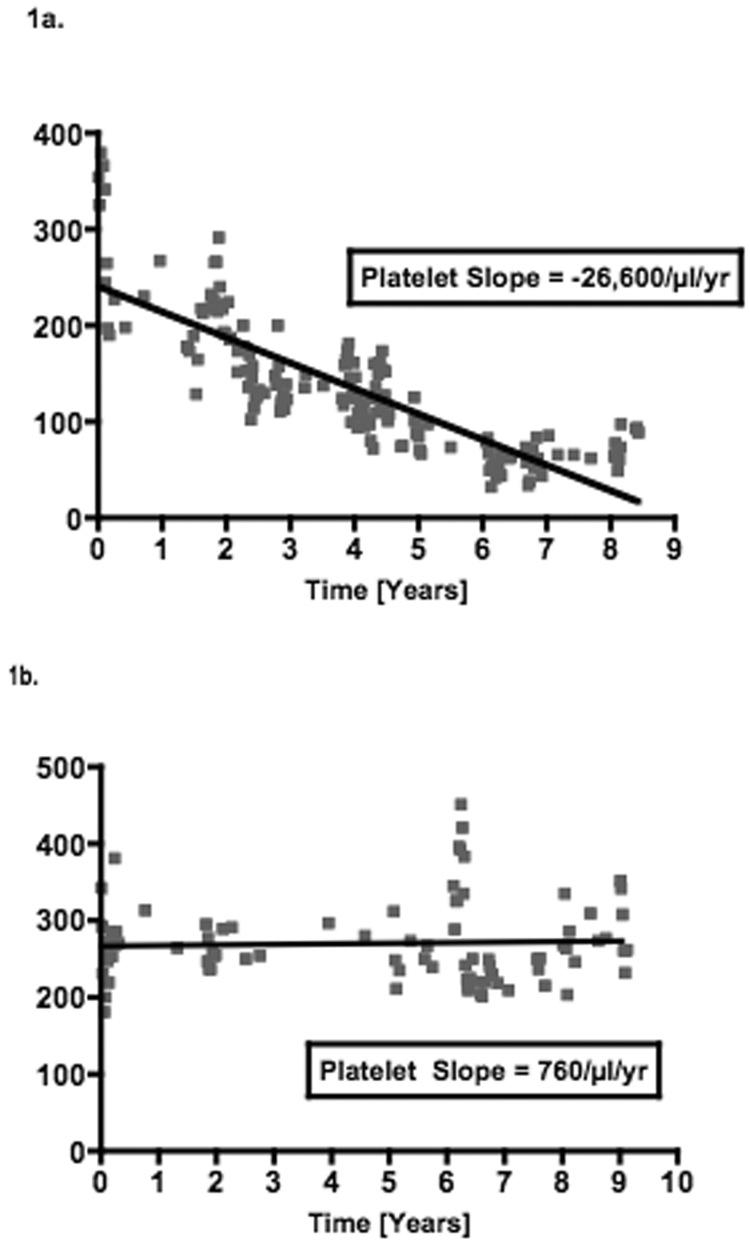
Conclusions: These data suggest mortality in patients with CGD is associated with the development of noncirrhotic portal hypertension, likely owing to injury to the microvasculature of the liver from repeated systemic and hepatic infections. The slope of decline in platelet count may be a useful measure of progression of portal hypertension over time. Furthermore, the data illustrate the potential independent effect of portal hypertension on clinical outcome outside the setting of cirrhosis.
Figures

Similar articles
-
Hepatic abnormalities in patients with chronic granulomatous disease.Hepatology. 2007 Mar;45(3):675-83. doi: 10.1002/hep.21524. Hepatology. 2007. PMID: 17326162
-
Acute portal hypertension associated with liver resection. Analysis of early postoperative death.Arch Surg. 1985 Nov;120(11):1303-5. doi: 10.1001/archsurg.1985.01390350083017. Arch Surg. 1985. PMID: 4051735
-
von Willebrand factor as new noninvasive predictor of portal hypertension, decompensation and mortality in patients with liver cirrhosis.Hepatology. 2012 Oct;56(4):1439-47. doi: 10.1002/hep.25806. Epub 2012 Aug 27. Hepatology. 2012. PMID: 22532296
-
Gastrointestinal and Hepatic Manifestations of Chronic Granulomatous Disease.J Allergy Clin Immunol Pract. 2023 May;11(5):1401-1416. doi: 10.1016/j.jaip.2022.12.039. Epub 2023 Jan 13. J Allergy Clin Immunol Pract. 2023. PMID: 36646382 Review.
-
Intrahepatic portal venopathy and related disorders of the liver.Semin Liver Dis. 2008 Aug;28(3):270-81. doi: 10.1055/s-0028-1085095. Epub 2008 Sep 23. Semin Liver Dis. 2008. PMID: 18814080 Review.
Cited by
-
Recent advances in transplantation for primary immune deficiency diseases: a comprehensive review.Clin Rev Allergy Immunol. 2014 Apr;46(2):131-44. doi: 10.1007/s12016-013-8379-6. Clin Rev Allergy Immunol. 2014. PMID: 23832379 Review.
-
Differential Diagnosis: Hepatic Complications in Inborn Errors of Immunity.J Clin Med. 2023 Dec 3;12(23):7480. doi: 10.3390/jcm12237480. J Clin Med. 2023. PMID: 38068532 Free PMC article. Review.
-
Noncirrhotic portal hypertension: An overview.Clin Liver Dis (Hoboken). 2015 Sep 29;6(3):72-74. doi: 10.1002/cld.497. eCollection 2015 Sep. Clin Liver Dis (Hoboken). 2015. PMID: 31040992 Free PMC article. No abstract available.
-
Granulomatous liver disease.Curr Gastroenterol Rep. 2009 Feb;11(1):42-9. doi: 10.1007/s11894-009-0007-5. Curr Gastroenterol Rep. 2009. PMID: 19166658 Review.
-
Reduced nicotinamide adenine dinucleotide phosphate oxidase 2 plays a key role in stellate cell activation and liver fibrogenesis in vivo.Gastroenterology. 2010 Oct;139(4):1375-84. doi: 10.1053/j.gastro.2010.05.074. Epub 2010 Jun 1. Gastroenterology. 2010. PMID: 20685364 Free PMC article.
References
-
- Jurkowska M, Bernatowska E, Bal J. Genetic and biochemical background of chronic granulomatous disease. Arch Immunol Ther Exp (Warsz) 2004;52:113–120. - PubMed
-
- Heyworth PG, Cross AR, Curnutte JT. Chronic granulomatous disease. Curr Opin Immunol. 2003;15:578–584. - PubMed
-
- Johnston RB., Jr Clinical aspects of chronic granulomatous disease. Curr Opin Hematol. 2001;8:17–22. - PubMed
-
- Marciano BE, Wesley R, De Carlo ES, Anderson VL, Barnhart LA, Darnell D, Malech HL, Gallin JI, Holland SM. Long-term interferon-gamma therapy for patients with chronic granulomatous disease. Clin Infect Dis. 2004;39:692–699. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
