

Chest sonography: a useful tool to differentiate acute cardiogenic pulmonary edema from acute respiratory distress syndrome
- PMID: 18442425
- PMCID: PMC2386861
- DOI: 10.1186/1476-7120-6-16
Chest sonography: a useful tool to differentiate acute cardiogenic pulmonary edema from acute respiratory distress syndrome
Abstract
Background: Differential diagnosis between acute cardiogenic pulmonary edema (APE) and acute lung injury/acute respiratory distress syndrome (ALI/ARDS) may often be difficult. We evaluated the ability of chest sonography in the identification of characteristic pleuropulmonary signs useful in the diagnosis of ALI/ARDS and APE.
Methods: Chest sonography was performed on admission to the intensive care unit in 58 consecutive patients affected by ALI/ARDS or by acute pulmonary edema (APE).
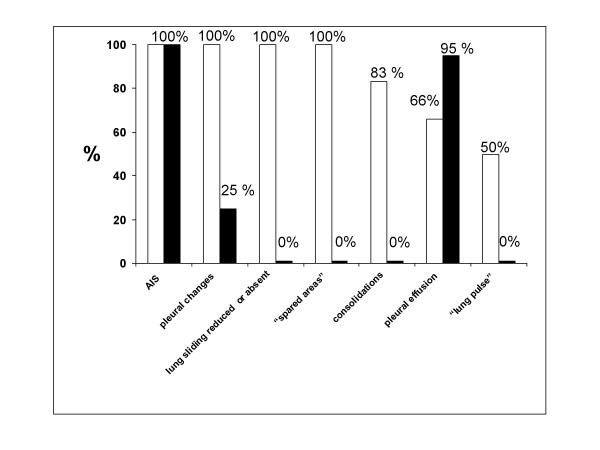
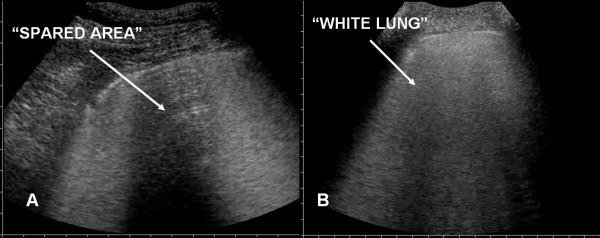
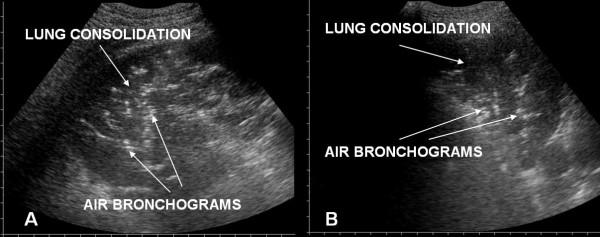
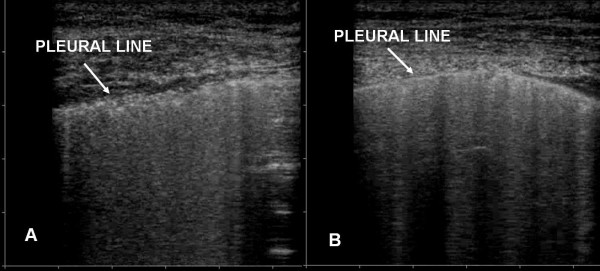
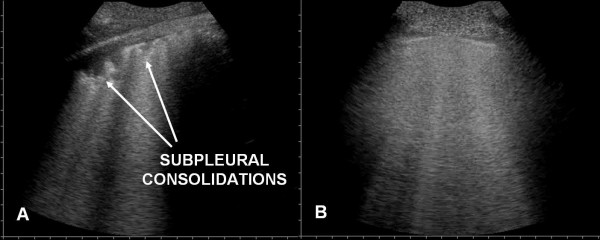
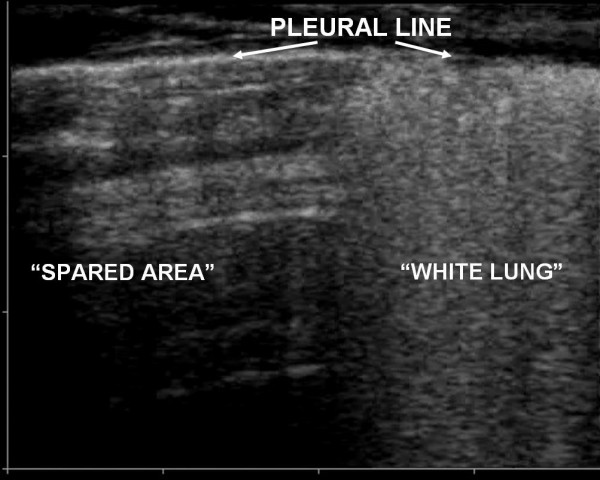
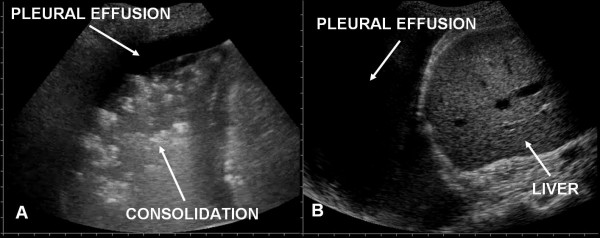
Results: Ultrasound examination was focalised on finding in the two groups the presence of: 1) alveolar-interstitial syndrome (AIS) 2) pleural lines abnormalities 3) absence or reduction of "gliding" sign 4) "spared areas" 5) consolidations 6) pleural effusion 7) "lung pulse".AIS was found in 100% of patients with ALI/ARDS and in 100% of patients with APE (p = ns). Pleural line abnormalities were observed in 100% of patients with ALI/ARDS and in 25% of patients with APE (p < 0.0001). Absence or reduction of the 'gliding sign' was observed in 100% of patients with ALI/ARDS and in 0% of patients with APE. 'Spared areas' were observed in 100% of patients with ALI/ARDS and in 0% of patients with APE (p < 0.0001). Consolidations were present in 83.3% of patients with ALI/ARDS in 0% of patients with APE (p < 0.0001). A pleural effusion was present in 66.6% of patients with ALI/ARDS and in 95% of patients with APE (p < 0.004). 'Lung pulse' was observed in 50% of patients with ALI/ARDS and in 0% of patients with APE (p < 0.0001). All signs, except the presence of AIS, presented a statistically significant difference in presentation between the two syndromes resulting specific for the ultrasonographic characterization of ALI/ARDS.
Conclusion: Pleuroparenchimal patterns in ALI/ARDS do find a characterization through ultrasonographic lung scan. In the critically ill the ultrasound demonstration of a dyshomogeneous AIS with spared areas, pleural line modifications and lung consolidations is strongly predictive, in an early phase, of non-cardiogenic pulmonary edema.
Figures
References
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R. The American European consensus conference on ARDS: definitions mechanisms, relevant outcomes and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–824. - PubMed
-
- Gattinoni L, Caironi P, Pelosi P, Goodman LR. What has computed tomography taught us about the acute respiratory distress syndrome? Am J Respir Crit Care Med. 2001;164:1701–11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
