

Long-term effects of renin-angiotensin system-blocking therapy and a low blood pressure goal on progression of hypertensive chronic kidney disease in African Americans
- PMID: 18443258
- PMCID: PMC3870204
- DOI: 10.1001/archinte.168.8.832
Long-term effects of renin-angiotensin system-blocking therapy and a low blood pressure goal on progression of hypertensive chronic kidney disease in African Americans
Abstract
Background: Antihypertensive drugs that block the renin-angiotensin system (angiotensin-converting enzyme inhibitors [ACEIs] or angiotensin receptor blockers) are recommended for patients with chronic kidney disease (CKD). A low blood pressure (BP) goal (BP, <130/80 mm Hg) is also recommended. The objective of this study was to determine the long-term effects of currently recommended BP therapy in 1094 African Americans with hypertensive CKD.
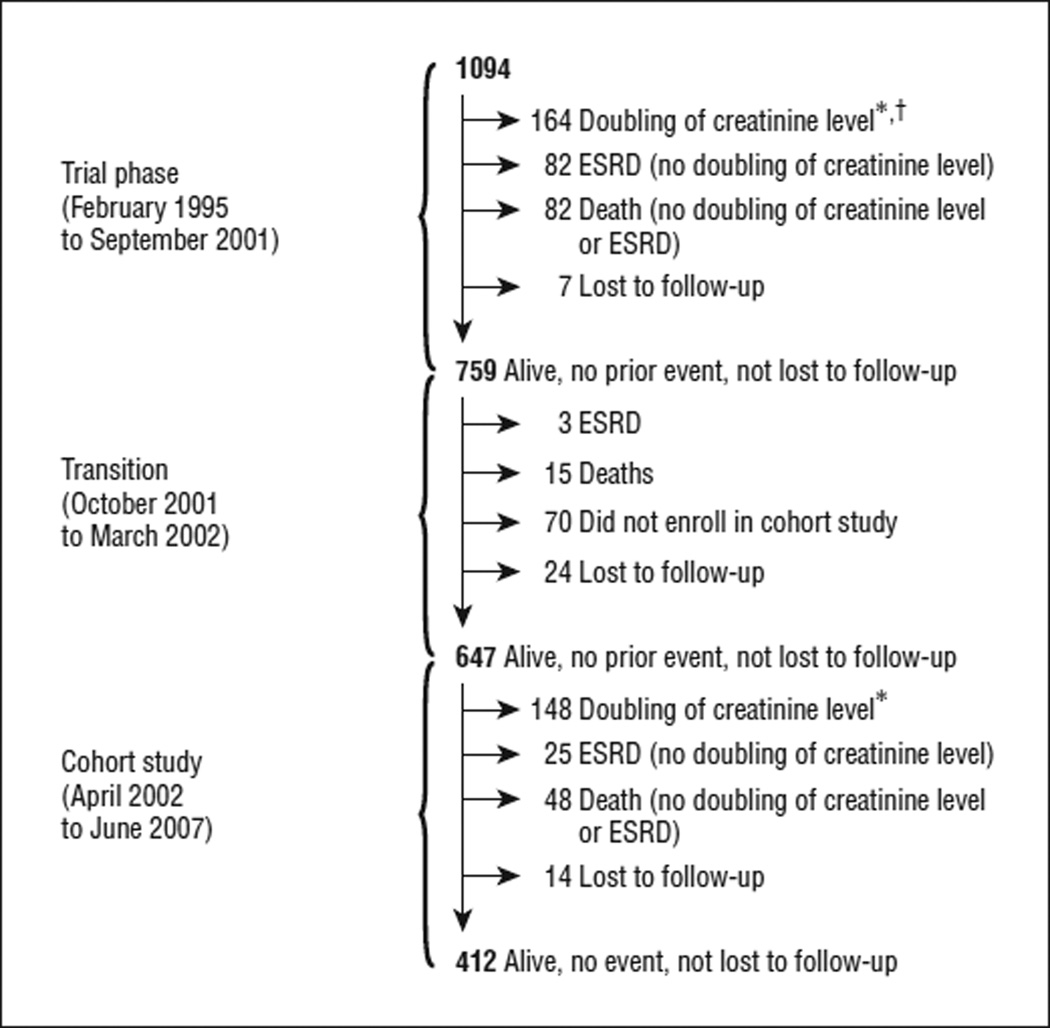
Methods: Multicenter cohort study following a randomized trial. Participants were 1094 African Americans with hypertensive renal disease (glomerular filtration rate, 20-65 mL/min/1.73 m2). Following a 3x2-factorial trial (1995-2001) that tested 3 drugs used as initial antihypertensive therapy (ACEIs, calcium channel blockers, and beta-blockers) and 2 levels of BP control (usual and low), we conducted a cohort study (2002-2007) in which participants were treated with ACEIs to a BP lower than 130/80 mm Hg. The outcome measures were a composite of doubling of the serum creatinine level, end-stage renal disease, or death.
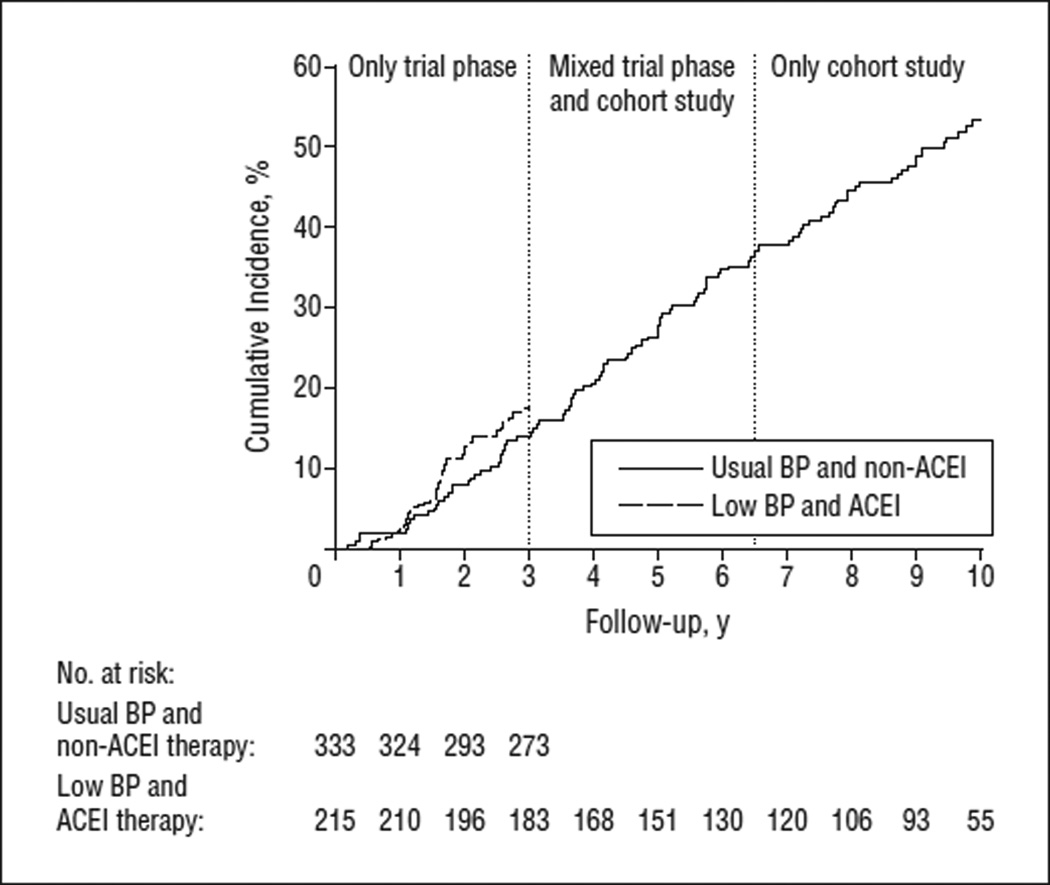
Results: During each year of the cohort study, the annual use of an ACEI or an angiotensin receptor blocker ranged from 83.7% to 89.0% (vs 38.5% to 49.8% during the trial). The mean BP in the cohort study was 133/78 mm Hg (vs 136/82 mm Hg in the trial). Overall, 567 participants experienced the primary outcome; the 10-year cumulative incidence rate was 53.9%. Of 576 participants with at least 7 years of follow-up, 33.5% experienced a slow decline in kidney function (mean annual decline in the estimated glomerular filtration rate, <1 mL/min/1.73 m2).
Conclusion: Despite the benefits of renin-angiotensin system-blocking therapy on CKD progression, most African Americans with hypertensive CKD who are treated with currently recommended BP therapy continue to progress during the long term.
Figures

Comment in
-
Should a lower blood pressure goal and albuminuria reduction be mandated to slow hypertensive nephropathy?Curr Hypertens Rep. 2008 Oct;10(5):387-8. Curr Hypertens Rep. 2008. PMID: 18775116 No abstract available.
-
RAAS blockade, renal failure, ESRD, and death among African Americans in the AASK Posttrial Cohort Study.Arch Intern Med. 2008 Nov 24;168(21):2383-4. doi: 10.1001/archinternmed.2008.510. Arch Intern Med. 2008. PMID: 19029505 No abstract available.
References
-
- Coresh J, Wei GL, McQuillan G, et al. Prevalence of high blood pressure and elevated serum creatinine level in the United States: findings from the Third National Health and Nutrition Examination Survey (1988–1994) Arch Intern Med. 2001;161(9):1207–1216. - PubMed
-
- U.S. Renal Data System, USRDS 2005 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; 2005.
-
- Rostand SG, Brown G, Kirk KA, Rutsky EA, Dustan HP. Renal insufficiency in treated essential hypertension. N Engl J Med. 1989;320(11):684–688. - PubMed
-
- Walker WG, Neaton JD, Cutler JA, Neuwirth R, Cohen JD. MRFIT Research Group. Renal function change in hypertensive members of the Multiple Risk Factor Intervention Trial: racial and treatment effects. JAMA. 1992;268(21):3085–3091. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, et al. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42(6):1206–1252. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
