

T2* and FSE MRI distinguishes four subtypes of neurodegeneration with brain iron accumulation
- PMID: 18443312
- PMCID: PMC2706154
- DOI: 10.1212/01.wnl.0000310985.40011.d6
T2* and FSE MRI distinguishes four subtypes of neurodegeneration with brain iron accumulation
Abstract
Background: Neurodegeneration with brain iron accumulation (NBIA) defines a group of genetic disorders characterized by brain iron deposition and associated with neuronal death. The known causes of NBIA include pantothenate kinase-associated neurodegeneration (PKAN), neuroferritinopathy, infantile neuroaxonal dystrophy (INAD), and aceruloplasminemia.
Objective: To define the radiologic features of each NBIA subtype.
Methods: Brain MRIs from patients with molecularly confirmed PKAN (26 cases), neuroferritinopathy (21 cases), INAD (four cases), and aceruloplasminemia (10 cases) were analyzed blindly to delineate patterns of iron deposition and neurodegeneration.
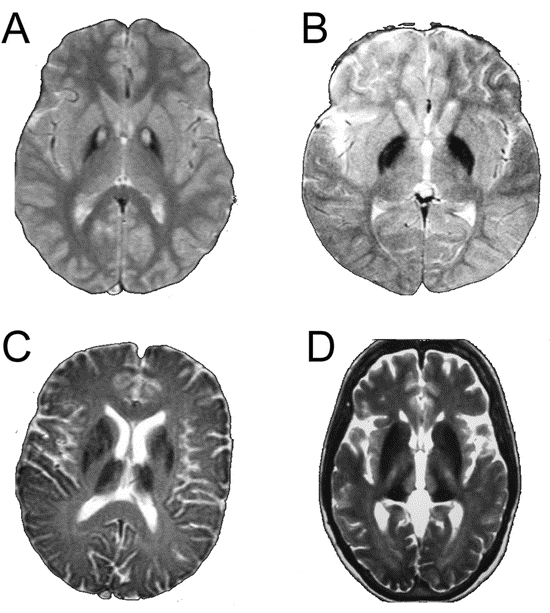
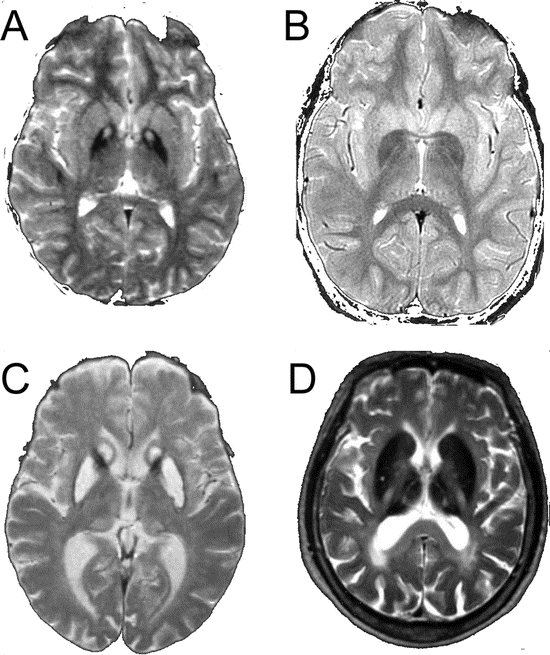
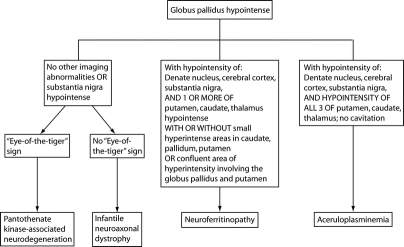
Results: In most cases of PKAN, abnormalities were restricted to globus pallidus and substantia nigra, with 100% having an eye of the tiger sign. In a minority of PKAN cases there was hypointensity of the dentate nuclei (1/5 on T2* sequences, 2/26 on fast spin echo [FSE]). In INAD, globus pallidus and substantia nigra were involved on T2* and FSE scans, with dentate involvement only seen on T2*. By contrast, neuroferritinopathy had consistent involvement of the dentate nuclei, globus pallidus, and putamen, with confluent areas of hyperintensity due to probable cavitation, involving the pallida and putamen in 52%, and a subset having lesions in caudate nuclei and thalami. More uniform involvement of all basal ganglia and the thalami was typical in aceruloplasminemia, but without cavitation.
Conclusions: In the majority of cases, different subtypes of neurodegeneration associated with brain iron accumulation can be reliably distinguished with T2* and T2 fast spin echo brain MRI, leading to accurate clinical and subsequent molecular diagnosis.
Figures

References
-
- Gelman N, Gorell JM, Barker PB, et al. MR imaging of human brain at 3.0 T: preliminary report on transverse relaxation rates and relation to estimated iron content. Radiology 1999;210:759–767. - PubMed
-
- Gerlach M, Double KL, Youdim MB, Riederer P. Potential sources of increased iron in the substantia nigra of parkinsonian patients. J Neural Transm Suppl 2006;70:133–142. - PubMed
-
- House MJ, St Pierre TG, Kowdley KV, et al. Correlation of proton transverse relaxation rates (R2) with iron concentrations in postmortem brain tissue from Alzheimer’s disease patients. Magn Reson Med 2007;57:172–180. - PubMed
-
- Hayflick SJ. Neurodegeneration with brain iron accumulation: from genes to pathogenesis. Semin Pediatr Neurol 2006;13:182–185. - PubMed
-
- Hayflick SJ, Westaway SK, Levinson B, et al. Genetic, clinical, and radiographic delineation of Hallervorden-Spatz syndrome. N Engl J Med 2003;348:33–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous