

A randomized, double-blind, crossover comparison of the efficacy and safety of oral controlled-release tramadol and placebo in patients with painful osteoarthritis
- PMID: 18443671
- PMCID: PMC2671217
- DOI: 10.1155/2008/165421
A randomized, double-blind, crossover comparison of the efficacy and safety of oral controlled-release tramadol and placebo in patients with painful osteoarthritis
Abstract
Objective: To compare the efficacy and safety of controlled-release (CR) tramadol (Zytram XL, Purdue Pharma, Canada) and placebo in patients with painful osteoarthritis.
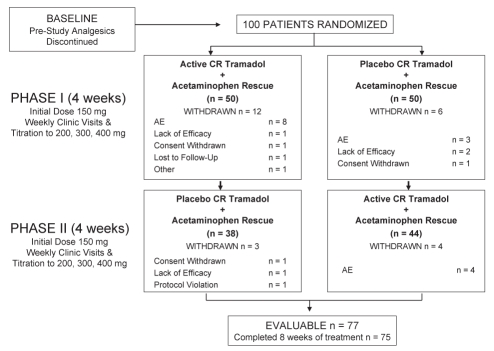
Methods: Patients underwent analgesic washout for two to seven days before random assignment to 150 mg daily of CR tramadol or placebo, and were titrated weekly to 200 mg, 300 mg or a maximum of 400 mg once daily. After four weeks, patients crossed over to the alternate treatment for another four weeks. Plain acetaminophen was provided as a rescue analgesic. All patients who completed the crossover study were eligible to receive open label CR tramadol for six months.
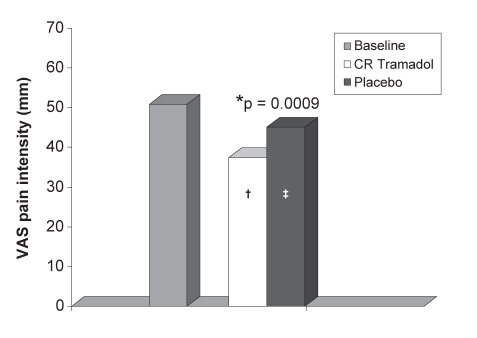
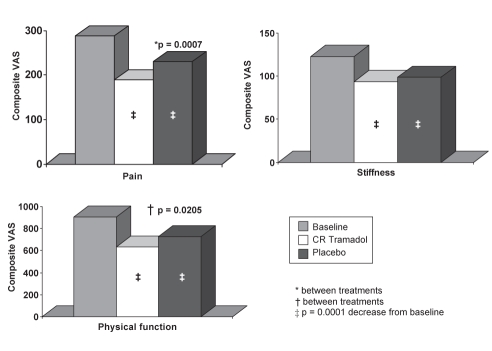
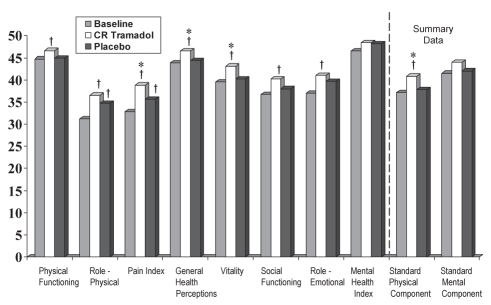
Results: Seventy-seven of 100 randomly assigned patients were evaluable for efficacy. CR tramadol resulted in significantly lower visual analogue scale pain intensity scores (37.4+/-23.9 versus 45.1+/-24.3, P=0.0009). Western Ontario and McMaster Universities osteoarthritis index subscale scores for pain (189.0+/-105.0 versus 230.0+/-115.4; P=0.0001) and physical function (632.4+/-361.3 versus 727.4+/-383.4; P=0.0205) were significantly better with CR tramadol. Total pain and disability (22.8+/-14.5 versus 27.2+/-14.8; P=0.0004), and overall pain and sleep (104.7+/-98.0 versus 141.0+/-108.2; P=0.0005) scores in the Pain and Sleep Questionnaire were significantly lower for CR tramadol. Short-form 36 Health Survey scores were significantly better during CR tramadol treatment for the pain index (38.8+/-10.8 versus 35.6+/-9.0; P=0.0100), general health perception (46.5+/-11.2 versus 44.4+/-11.6; P=0.0262), vitality (43.1+/-13.2 versus 40.2+/-13.7; P=0.0255) and overall physical components (40.8+/-8.9 versus 37.8+/-7.7; P=0.0002). CR tramadol treatment was preferred by 55.8% of patients (P=0.0005) versus 20.8% and 23.4% of patients who chose placebo or had no preference, respectively. These improvements were sustained for up to six months, and 86.5% of patients reported at least moderate benefit from CR tramadol during long-term treatment.
Conclusion: CR tramadol is effective for the management of painful osteoarthritis.
OBJECTIF :: Comparer l’efficacité et l’innocuité du tramadol à libération contrôlée (TLC) (Zytram XL, Purdue Pharma, Canada) et d’un placebo chez des patients souffrant d’arthrose douloureuse.
MÉTHODOLOGIE :: Les patients ont subi un sevrage de leurs analgésiques pendant deux à sept jours avant d’être répartis de manière aléatoire entre un traitement de 150 mg de TLC et un placebo, et ils ont été titrés toutes les semaines à 200 mg, 300 mg ou un maximum de 400 mg une fois par jour. Au bout de quatre semaines, les patients sont passés à l’autre traitement, de nouveau pendant quatre semaines. Le simple acétaminophène servait d’analgésique de rattrapage. Tous les patients qui terminaient l’étude croisée étaient admissibles à recevoir un traitement ouvert au TLC pendant six mois.
RÉSULTATS :: Soixante-dix-sept des 100 patients divisés au hasard pouvaient faire l’objet d’une évaluation d’efficacité. Selon l’échelle visuelle analogique, le TLC s’associait à une diminution considérable de l’intensité de la douleur (37,4±23,9 par rapport à 45,1±24,3, P=0,0009). Les indices des sous-échelles de la douleur de l’université de Western Ontario et de l’université McMaster (189,0±105,0 par rapport à 230,0±115,4, P=0,0001) et la fonction physique (632,4,0±361,3 par rapport à 727,4±383,4, P=0,0205) s’amélioraient de manière significative avec le TLC. Les indices de douleur totale et d’incapacité (22,8±14,5 par rapport à 27,2±14,8, P=0,0004) et de douleur globale et de sommeil (104,7±98,0 par rapport à 141,0±108,2, P=0,0005) du questionnaire sur la douleur et le sommeil étaient beaucoup plus faibles pour le TLC. Les indices du questionnaire court en 36 questions étaient beaucoup plus positifs pendant le traitement au TLC pour ce qui est de l’indice de la douleur (38,8±10,8 par rapport à 35,6±9,0, P=0,0100), de la perception de santé générale (46,5±11,2 par rapport à 44,4±11,6, P=0,0262), de la vitalité (43,1±13,2 par rapport à 40,2±13,7, P=0,0255) et des éléments physiques globaux (40,8±8,9 par rapport à 37,8±7,7, P=0,0002). Le traitement au TLC était préféré par 55,8 % des patients (P=0,0005) par rapport à 20,8 % et 23,4 % de ceux qui prenaient un placebo ou qui n’avaient pas de préférence, respectivement. Ces améliorations étaient maintenues jusqu’à six mois, et 86,5 % des patients déclaraient au moins des bienfaits modérés du TLC pendant le traitement prolongé.
CONCLUSION :: Le TLC est efficace pour la prise en charge de l’arthrose douloureuse.
Figures
Comment in
-
Re: Beaulieu AD, Peloso PM, Haraoui B, et al. Once-daily, controlled-release tramadol and sustained-release diclofenac relieve chronic pain to to osteoarthritis: a randomized controlled trial. Pain Res Manage 2008; 13:103-10, and Thorne C, Beaulieu AD, Callaghan DJ, et. al. A randomized, double-blind, crossover comparison of the efficacy and safety of oral controlled-release tramadol and placebo in patients with painful osteoarthritis. Pain Res Manage 2008; 13:93-102.Pain Res Manag. 2008 Jul-Aug;13(4):342. doi: 10.1155/2008/181659. Pain Res Manag. 2008. PMID: 18816899 Free PMC article. No abstract available.
References
-
- Health Canada. Arthritis in Canada. An ongoing challenge. <http://www.phac-aspc.gc.ca/publicat/ac/pdf/ac_e.pdf> (Version current at March 18, 2008).
-
- Breedveld FC. Osteoarthritis – the impact of a serious disease. Rheumatology (Oxford) 2004;43(Suppl 1):i4–8. - PubMed
-
- Liang MH, Fortin P. Management of osteoarthritis of the hip and knee. N Engl J Med. 1991;325:125–7. - PubMed
-
- Gupta S, Hawker GA, Laporte A, Croxford R, Coyte PC. The economic burden of disabling hip and knee osteoarthritis (OA) from the perspective of individuals living with this condition. Rheumatology (Oxford) 2005;44:1531–7. - PubMed
-
- World Health Organization . Cancer Pain Relief, With a guide to opioid availability. 2nd ed. Geneva: World Health Organization; 1996.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
