

Delayed sleep phase cases and controls
- PMID: 18445295
- PMCID: PMC2391143
- DOI: 10.1186/1740-3391-6-6
Delayed sleep phase cases and controls
Abstract
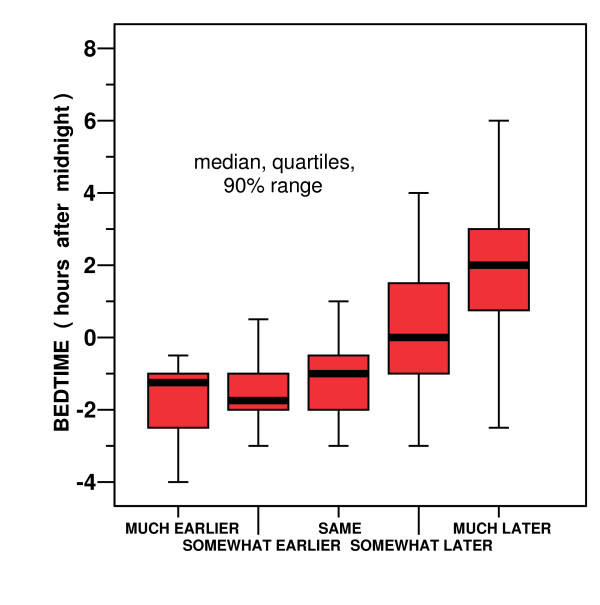
Background: Delayed sleep phase disorder (DSPD) is a condition in which patients have difficulty falling asleep before the early morning hours and commonly have trouble awakening before late morning or even early afternoon. Several studies have suggested that variations in habitual bedtime are 40-50% heritable.
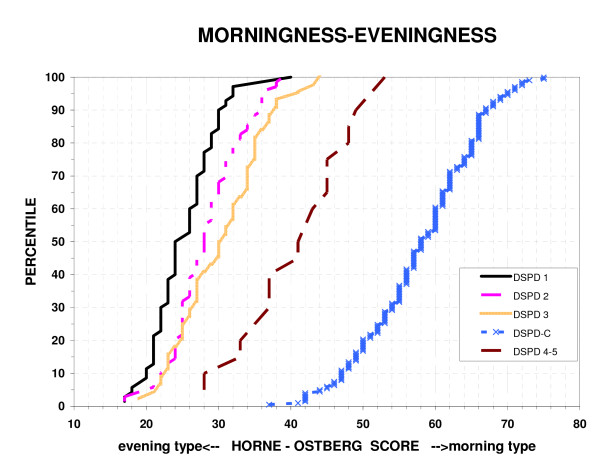
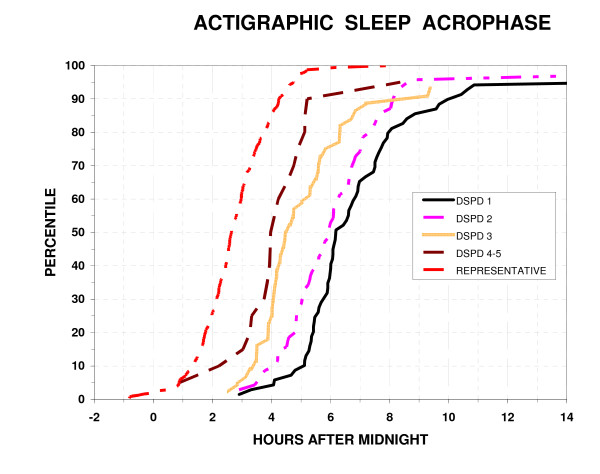
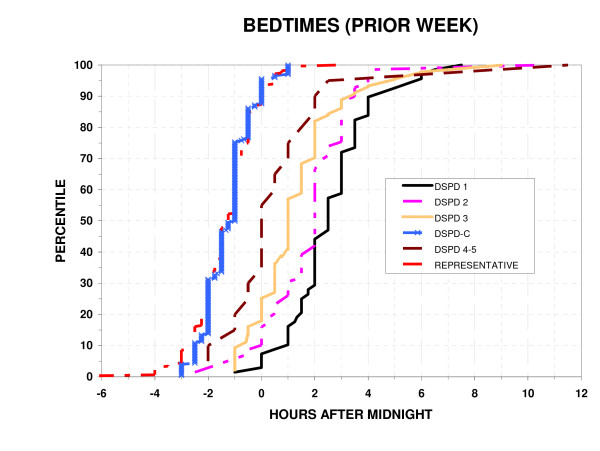
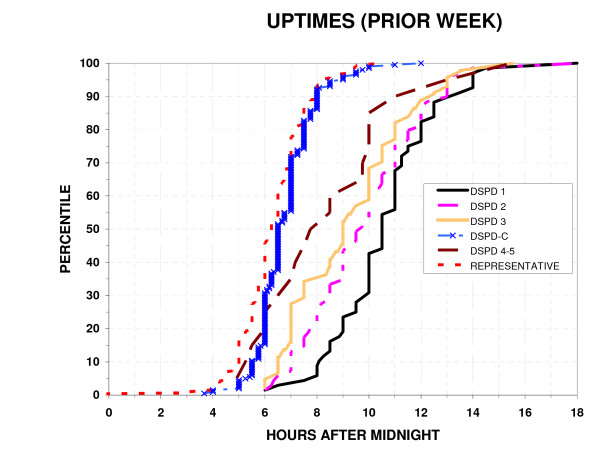
Methods: We recruited a case series of 205 participants, along with 221 controls (DSPD-C) with normal sleep, roughly matched for age, gender, and ancestry. A representative sample of San Diego adults recruited some years before was already available to confirm the control group. Both DSPD and DSPD-C provided blood or saliva samples for DNA and completed extensive questionnaires about sleep habits, sleep history, family history, sleep quality, morningness-eveningness traits, depression, mania, and seasonality of symptoms. The DSPD group wore wrist actigraphs for a median of 13.2 days. The representative sample collected previously had undergone actigraphic recordings, from which 48 hours of data were generally available.
Results: The DSPD and DSPD-C samples showed almost no overlap on morningness-eveningness scores. DSPD cases went to bed and arose about 3 hours later than the DSPD-C and the representative sample. DSPD cases reported more difficulties with sleep, poorer sleep quality, and more depression, but there was no significant difference in a history of mania. DSPD cases reported more family history of late bedtimes, but female DSPD reported that their fathers' bedtimes were later than the fathers of male DSPD.
Conclusion: These results indicate a DSPD phenotype is familial and associated with unipolar depression.
Figures
References
-
- Horne JA, Östberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4:97–110. - PubMed
-
- Winkelman J, Kotagal S, Olson E, Scammel T, Schenck C, Spielman A. The International Classification of Sleep Disorders, Second Edition, Pocket Version: Diagnostic and Coding Manual. Westchester, IL, American Academy of Sleep Disorders; 2006.
-
- Schrader H, Bovim G, Sand T. The prevalence of delayed and advanced sleep phase syndrome. J Sleep Res. 1993;2:51–55. - PubMed
-
- Ando K, Kripke DF, Ancoli-Israel S. Delayed and advanced sleep phase symptoms. Isr J Psychiatry Relat Sci. 2002;39:11–18. - PubMed
