

Review
doi: 10.1007/s00330-008-0968-z.
Epub 2008 Apr 30.
Diffusion-weighted whole-body imaging with background body signal suppression (DWIBS): features and potential applications in oncology
Affiliations
- PMID: 18446344
- PMCID: PMC2516183
- DOI: 10.1007/s00330-008-0968-z
Item in Clipboard
Review
Diffusion-weighted whole-body imaging with background body signal suppression (DWIBS): features and potential applications in oncology
Eur Radiol.
2008 Sep.
Abstract
Diffusion-weighted magnetic resonance imaging (DWI) provides functional information and can be used for the detection and characterization of pathologic processes, including malignant tumors. The recently introduced concept of "diffusion-weighted whole-body imaging with background body signal suppression" (DWIBS) now allows acquisition of volumetric diffusion-weighted images of the entire body. This new concept has unique features different from conventional DWI and may play an important role in whole-body oncological imaging. This review describes and illustrates the basics of DWI, the features of DWIBS, and its potential applications in oncology.
Figures
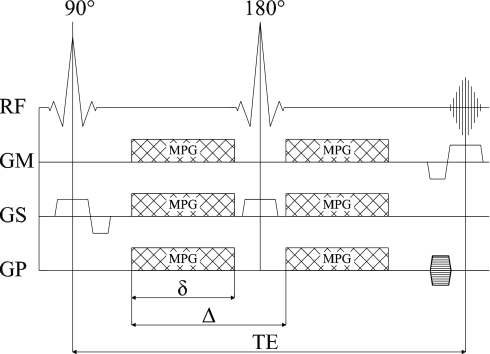
The Stejskal-Tanner sequence [5] (RF radio frequency, GM readout direction, GP phase encoding direction, GS section select direction, MPG motion probing gradient, δ duration of one MPG, Δ time interval between the leading edges of the MPGs, TE echo time)
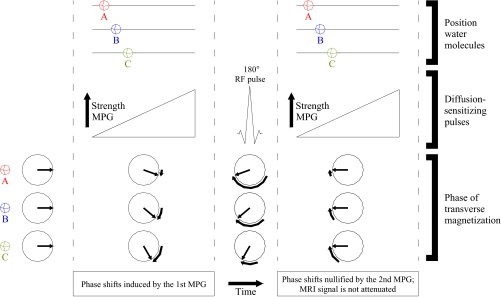
Three stationary water molecules (A, B, C) in one voxel. Phase shifts induced by the first motion probing gradient (MPG) are nullified by the second MPG. Because of the maintained phase coherence among the three water molecules, the MRI signal is not attenuated (RF radio frequency)
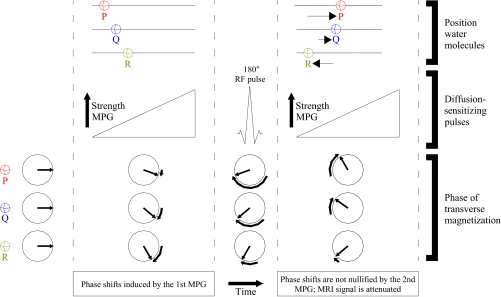
Three water molecules (P, Q, R) in one voxel, undergoing diffusion. Phase shifts induced by the first motion probing gradient (MPG) are not nullified by the second MPG. Because of the resulting phase dispersion among the three water molecules, the MRI signal is attenuated (RF radio frequency)

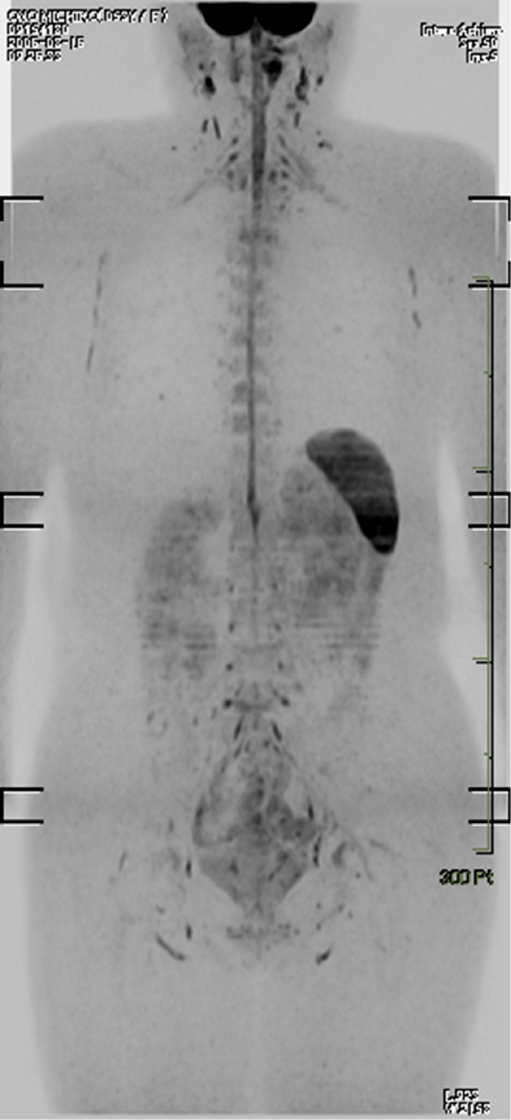
Coronal maximum intensity projection DWIBS image (inverted black-and-white gray scale) of a healthy 60-year-old male volunteer. Normal high signal intensity (black on this image) can be seen in the brain, spinal cord, nerves of the brachial plexus, prostate, testis, penis, spleen, and cervical, axillary, pelvic, and inguinal lymph nodes
Coronal maximum intensity projection DWIBS image (inverted black-and-white gray scale) of a healthy 53-year-old female volunteer. Normal high signal intensity (black on this image) can be seen in the brain, spinal cord, nerves of the brachial and lumbosacral plexus, vertebral bone marrow, endometrium, spleen, and cervical, axillary, pelvic, and inguinal lymph nodes

Three stationary water molecules (X, Y, Z) in one voxel, undergoing respiratory motion. Respiratory motion induces a linear phase shift but does not cause phase dispersion. Because of the maintained phase coherence among the three water molecules, MRI signal is preserved (MPG motion probing gradient, RF radio frequency)
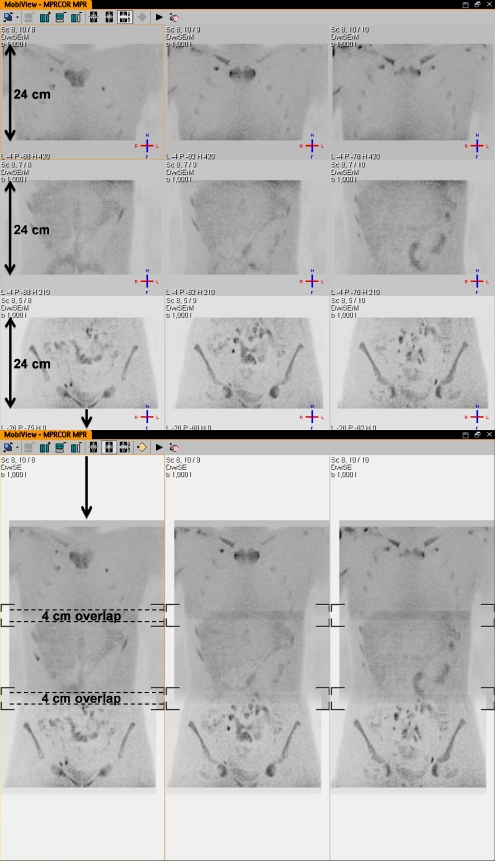
Separately imaged stations can be merged with sophisticated software, creating the whole-body image
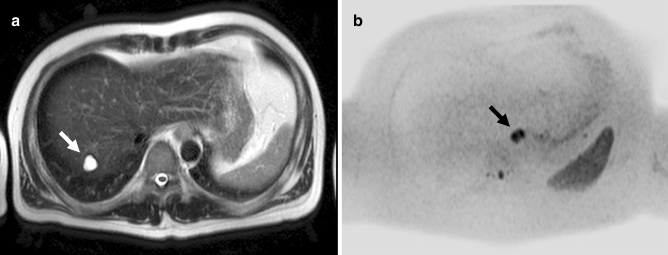
A 41-year-old man with distal esophageal cancer shown by DWIBS but inconspicuous on T2-weighted MRI. a Axial T2-weighted image shows a small high signal intensity lesion in segment 7 of the liver (arrow), consistent with a cyst. No other conspicuous lesions can be identified. b Axial DWIBS image (inverted black-and-white gray scale) at the same level shows abnormal signal intensity in the lower part of the esophagus (arrow), consistent with esophageal carcinoma
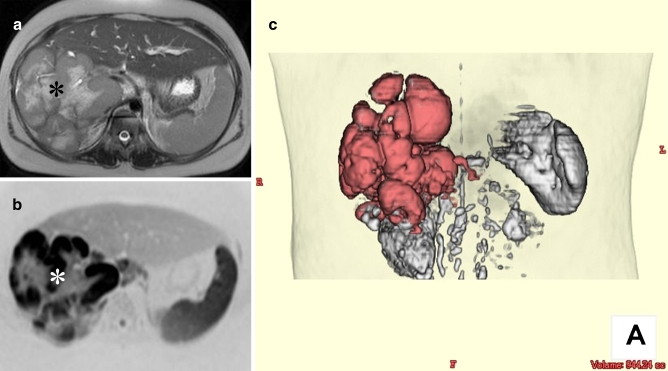
Volume measurement of a primary hepatic diffuse large B-cell lymphoma in a 10-year-old girl using DWIBS. a Axial respiratory-gated T2-weighted image shows a bulky mass occupying most of the right lobe of the liver (asterisk). b Axial DWIBS image (inverted black-and-white gray scale) at the same level clearly visualizes the tumor with excellent contrast between the tumor and surrounding tissue (asterisk). c Volume-rendered image using thin slice (4 mm, no gap) DWIBS dataset shows the three-dimensional shape of the tumor (colored red) and allows for tumor volume measurement

Comparison of pre- and post-chemotherapy FDG-PET and DWIBS images in a 44-year-old man with diffuse large B-cell lymphoma. a Coronal maximum intensity projection FDG-PET and b coronal maximum intensity projection DWIBS images before initiation of chemotherapy. Both images show cervical, bilateral supra/infraclavicular, mediastinal, left axillary, para-aortic lymph node, and splenic involvement (arrows), and cardiac involvement (dashed arrow). c FDG-PET and d DWIBS images at the end of treatment show resolvement of all pre-existing lesions. a, b A limitation of DWIBS is that discrimination between normal and metastatic lymph nodes is still based on size criteria; the FDG-PET positive left cervical lymph node (arrowhead 1) cannot conclusively be identified as malignant on DWIBS (arrowhead 1). DWIBS also shows prominent bilateral inguinal lymph nodes (encircled) which are normal according to FDG-PET. On the other hand, thanks to its higher spatial resolution, DWIBS visualizes two separate cardiac lesions (dashed arrow), whereas FDG-PET shows only one large cardiac lesion (dashed arrow). DWIBS also allows better evaluation of the urinary tract than FDG-PET, where potential lesions can be obscured because of FDG accumulation (arrowheads 2). c Note the physiological FDG uptake in the large intestine (arrow), which should not be confused with persistent malignant lymphoma

A 78-year-old man with metastatic lung cancer and two benign lesions visualized with DWIBS. Coronal maximum intensity projection DWIBS image shows an area with restricted diffusion in the right lower lobe, consistent with lung cancer (arrow). In addition, DWIBS image shows ipsilateral hilar lymph node metastasis (arrowhead 1), retroperitoneal/adrenal metastasis (arrowhead 2), and vertebral metastasis (arrowhead 3). DWIBS image also shows restricted diffusion in a thoracic vertebra (arrowhead A). T1- and T2-weighted images (not shown), however, indicate this “lesion” to be a (benign) cavernous hemangioma, instead of a vertebral metastasis. Furthermore, DWIBS image shows a well-circumscribed area of restricted diffusion in the epigastric region (arrowhead B); physical examination reveals a (benign) sebaceous cyst to be responsible for this area of restricted diffusion
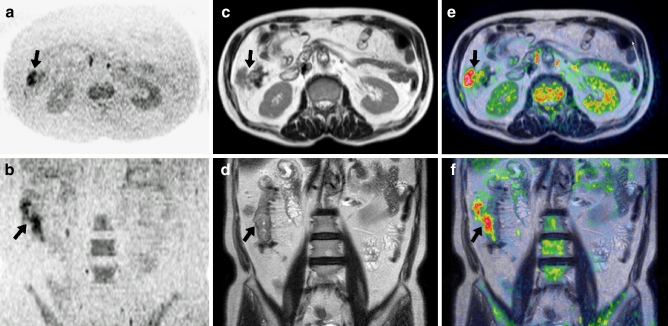
Fusion of a DWIBS image and a T2-weighted image in a 64-year-old man with ascending colon cancer. a Axial and b coronally reformatted DWIBS images show abnormal signal in the area of the ascending colon. c Axial and d coronal T2-weighted images show a large mass of intermediate signal intensity in the ascending colon, extending beyond the serosa. e Fused axial and f coronal DWIBS/T2-weighted images, highlighting the lesion
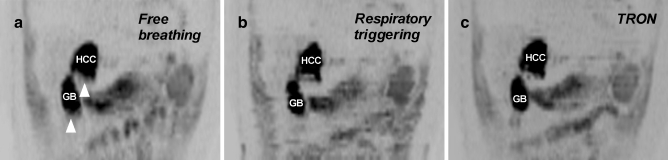
Comparison of DWIBS images obtained (1) during free breathing, (2) with respiratory triggering, and (3) with TRON, in a 48-year-old male with hepatocellular carcinoma and hemochromatosis. a Coronally reformatted DWIBS image obtained during free breathing shows an area with restricted diffusion in segment IV of the liver; biopsy proved this lesion to be a hepatocellular carcinoma (HCC). Bile in the gallbladder (GB) also shows restricted diffusion. Note significant blurring of the hepatocellular carcinoma and the gallbladder, especially at their lower boundaries (arrowheads). b Coronally reformatted DWIBS image obtained with respiratory triggering results in reduced blurring of the hepatocellular carcinoma (HCC) and the gallbladder (GB), but introduces stepladder-like artifacts due to gating error. Furthermore, image acquisition time is approximately 2.5-times prolonged in comparison with a. c Coronally reformatted DWIBS image obtained with TRON shows slight gating error, but offers good delineation of the hepatocellular carcinoma (HCC) and the gallbladder (GB). Image acquisition time is only slightly (approximately 1.2-times) increased in comparison with a
References
-
- World Health Organization . International union against cancer. Global action against cancer. Geneva: WHO Press; 2005.
-
- Ichikawa T, Haradome H, Hachiya J, Nitatori T, Araki T. Diffusion-weighted MR imaging with a single-shot echoplanar sequence: detection and characterization of focal hepatic lesions. AJR Am J Roentgenol. 1998;170:397–402. - PubMed
-
- Muller MF, Prasad P, Siewert B, et al. Abdominal diffusion mapping with use of a whole-body echo-planar system. Radiology. 1994;190:475–478. - PubMed
-
- Muller MF, Prasad P, Bimmler D, et al. Functional imaging of the kidney by means of measurement of the apparent diffusion coefficient. Radiology. 1994;193:711–715. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
