

Treatment of tendinopathy: what works, what does not, and what is on the horizon
- PMID: 18446422
- PMCID: PMC2505250
- DOI: 10.1007/s11999-008-0260-1
Treatment of tendinopathy: what works, what does not, and what is on the horizon
Abstract
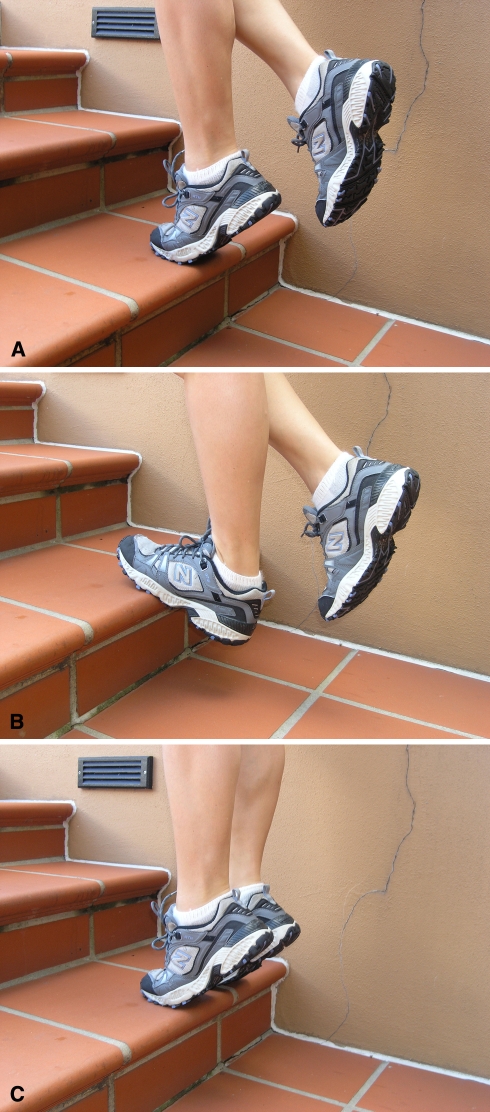
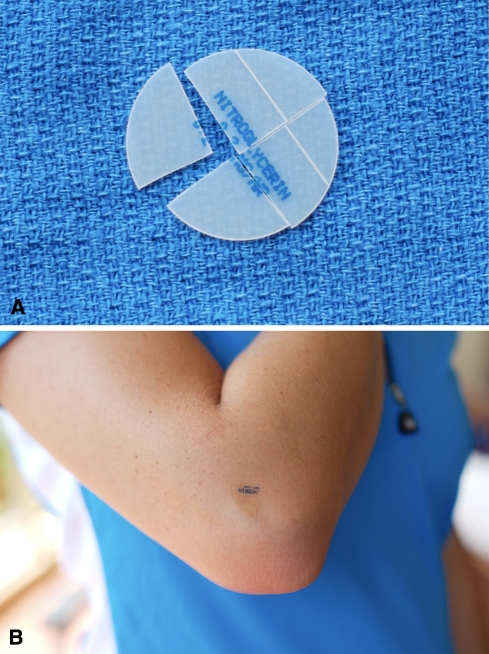
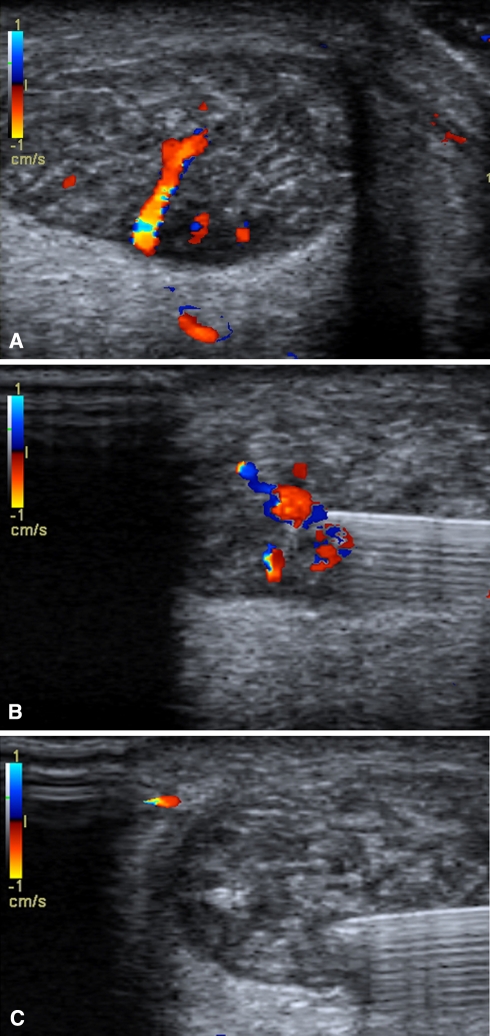
Tendinopathy is a broad term encompassing painful conditions occurring in and around tendons in response to overuse. Recent basic science research suggests little or no inflammation is present in these conditions. Thus, traditional treatment modalities aimed at controlling inflammation such as corticosteroid injections and nonsteroidal antiinflammatory medications (NSAIDS) may not be the most effective options. We performed a systematic review of the literature to determine the best treatment options for tendinopathy. We evaluated the effectiveness of NSAIDS, corticosteroid injections, exercise-based physical therapy, physical therapy modalities, shock wave therapy, sclerotherapy, nitric oxide patches, surgery, growth factors, and stem cell treatment. NSAIDS and corticosteroids appear to provide pain relief in the short term, but their effectiveness in the long term has not been demonstrated. We identified inconsistent results with shock wave therapy and physical therapy modalities such as ultrasound, iontophoresis and low-level laser therapy. Current data support the use of eccentric strengthening protocols, sclerotherapy, and nitric oxide patches, but larger, multicenter trials are needed to confirm the early results with these treatments. Preliminary work with growth factors and stem cells is promising, but further study is required in these fields. Surgery remains the last option due to the morbidity and inconsistent outcomes. The ideal treatment for tendinopathy remains unclear.
Level of evidence: Level II, systematic review.
Figures
References
-
- Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for shoulder pain. Phys Ther. 2001;81:1719–1730. - PubMed
-
- Adebajo AO, Nash P, Hazleman BL. A prospective double blind dummy placebo controlled study comparing triamcinolone hexacetonide injection with oral diclofenac 50 mg TDS in patients with rotator cuff tendinitis. J Rheumatol. 1990;17:1207–1210. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
