

Selective serotonin reuptake inhibitors for premenstrual syndrome and premenstrual dysphoric disorder: a meta-analysis
- PMID: 18448752
- PMCID: PMC2670364
- DOI: 10.1097/AOG.0b013e31816fd73b
Selective serotonin reuptake inhibitors for premenstrual syndrome and premenstrual dysphoric disorder: a meta-analysis
Abstract
Objective: To systematically review evidence of the treatment benefits of selective serotonin reuptake inhibitors (SSRIs) for symptoms related to severe premenstrual syndrome (PMS) and premenstrual dysphoric disorder.
Data sources: We conducted electronic database searches of MEDLINE, Web of Science, Cochrane Library, Embase, PsycINFO, and Cinahl through March 2007, and hand-searched reference lists and pertinent journals.
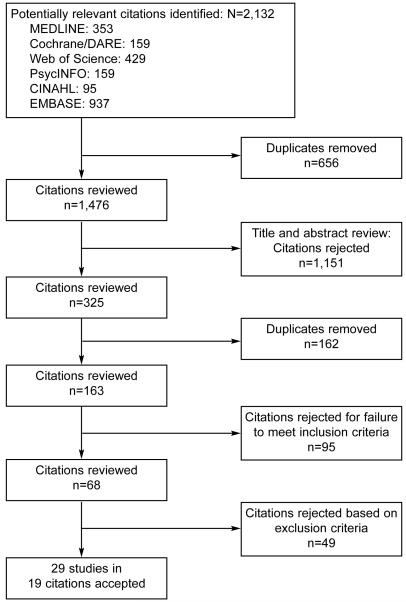
Methods of study selection: Studies included in the review were double-blind, randomized, controlled trials comparing an SSRI with placebo that reported a change in a validated score of premenstrual symptomatology. Studies had to report follow-up for any duration longer than one menstrual cycle among premenopausal women who met clinical diagnostic criteria for PMS or premenstrual dysphoric disorder. From 2,132 citations identified, we pooled results from 29 studies (in 19 citations) using random-effects meta-analyses and present results as odds ratios (ORs).
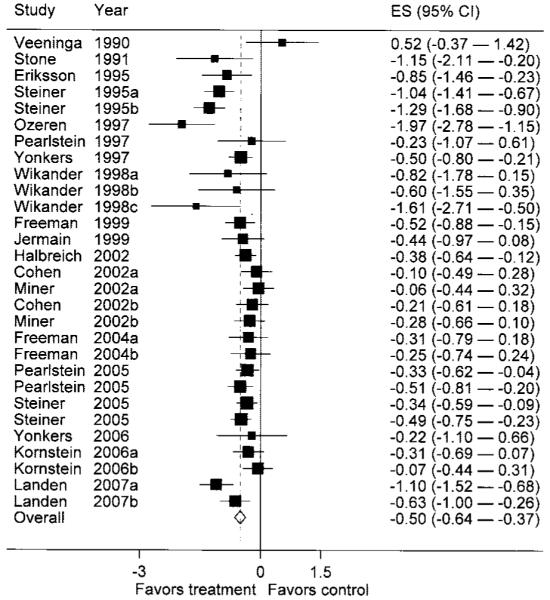
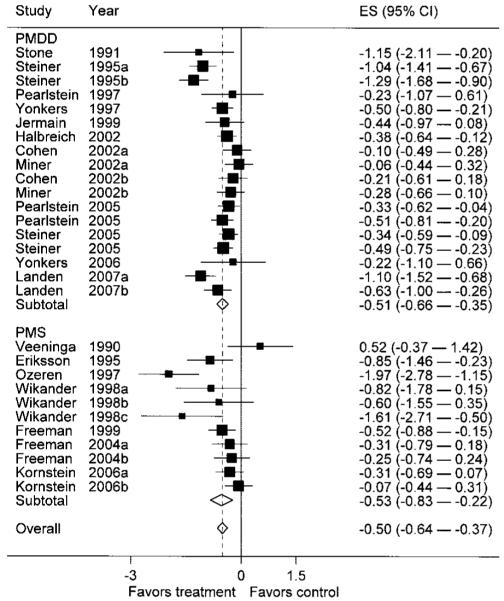
Tabulation, integration, and results: Our meta- analysis, which included 2,964 women, demonstrates that SSRIs are effective for treating PMS and premenstrual dysphoric disorder (OR 0.40, 95% confidence interval [CI] 0.31-0.51). Intermittent dosing regimens were found to be less effective (OR 0.55, 95% CI 0.45-0.68) than continuous dosing regimens (OR 0.28, 95% CI 0.18-0.42). No SSRI was demonstrably better than another. The choice of outcome measurement instrument was associated with effect size estimates. The overall effect size is smaller than reported previously.
Conclusion: Selective serotonin reuptake inhibitors were found to be effective in treating premenstrual symptoms, with continuous dosing regimens favored for effectiveness.
Figures
References
-
- Halbreich U, Borenstein J, Pearlstein T, Kahn LS. The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder (PMS/PMDD) Psychoneuroendocrinology. 2003;28(suppl):1–23. - PubMed
-
- Rapkin AJ. New treatment approaches for premenstrual disorders. Am J Manag Care. 2005;11:S480–91. - PubMed
-
- Steiner M, Pearlstein T, Cohen LS, Endicott J, Kornstein SG, Roberts C, et al. Expert guidelines for the treatment of severe PMS, PMDD, and comorbidities: the role of SSRIs. J Womens Health (Larchmt) 2006;15:57–69. - PubMed
-
- Inoue Y, Terao T, Iwata N, Okamoto K, Kojima H, Okamoto T, et al. Fluctuating serotonergic function in premenstrual dysphoric disorder and premenstrual syndrome: findings from neuroendocrine challenge tests. Psychopharmacology (Berl) 2007;190:213–9. - PubMed
-
- Dimmock PW, Wyatt KM, Jones PW, O’Brien PM. Efficacy of selective serotonin-reuptake inhibitors in premenstrual syndrome: a systematic review. Lancet. 2000;356:1131–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
