

Prevalence of musculoskeletal pain and statin use
- PMID: 18449611
- PMCID: PMC2517983
- DOI: 10.1007/s11606-008-0636-7
Prevalence of musculoskeletal pain and statin use
Abstract
Background: Muscle effects are the most common reported adverse effects of 3-hydroxy-3-methylglutaryl coenzyme A inhibitors (statins). However, in placebo-controlled trials the incidence of muscle pain is most often similar for placebo and active control groups.
Objective: We sought to evaluate whether statin use was associated with a higher prevalence of musculoskeletal pain in a nationally representative sample.
Methods: Cross-sectional analysis using data from the National Health and Nutrition Examination Survey (NHANES) 1999-2002. Participants were 3,580 adults > or =40 years without arthritis who were interviewed at home and examined in a mobile examination center. Participants were asked about sociodemographic characteristics, health conditions, medication use, and musculoskeletal pain. Height, weight, blood pressure, ankle brachial index, and cholesterol were measured.
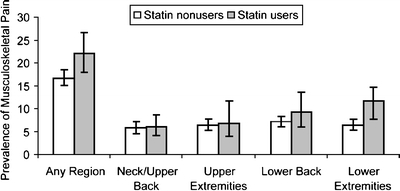
Measurements and main results: Prevalence and adjusted odds ratios (OR) of any musculoskeletal pain and musculoskeletal pain in 4 different anatomical regions (neck/upper back, upper extremities, lower back, and lower extremities) by statin use during the last 30 days. Among statin users (n = 402), 22.0% (95%CI 18.0-26.7%) reported musculoskeletal pain in at least 1 anatomical region during the last 30 days, compared with 16.7% (95%CI 15.1-18.4%) of those who did not use a statin. Compared to persons who did not use statins, those who used statins had multivariable-adjusted odds ratios (95%CI; p value) of 1.50 (1.07-2.11; p = .01) for any musculoskeletal pain, 1.59 (1.04-2.44, p = .03) for lower back pain, and 1.50 (1.02-2.22, p = .03) for lower extremity pain.
Conclusion: Musculoskeletal pain is common in adults > or =40 years without arthritis. In this nationally representative sample, statin users were significantly more likely to report musculoskeletal pain.
Figures
Similar articles
-
Statin use and musculoskeletal pain among adults with and without arthritis.Am J Med. 2012 Feb;125(2):176-82. doi: 10.1016/j.amjmed.2011.08.007. Am J Med. 2012. PMID: 22269621 Free PMC article.
-
Vitamin D status modifies the association between statin use and musculoskeletal pain: a population based study.Atherosclerosis. 2015 Jan;238(1):77-82. doi: 10.1016/j.atherosclerosis.2014.11.012. Epub 2014 Nov 20. Atherosclerosis. 2015. PMID: 25437894 Free PMC article.
-
Statins and musculoskeletal conditions, arthropathies, and injuries.JAMA Intern Med. 2013 Jul 22;173(14):1-10. doi: 10.1001/jamainternmed.2013.6184. JAMA Intern Med. 2013. PMID: 23877079
-
CoQ10 and L-carnitine for statin myalgia?Expert Rev Cardiovasc Ther. 2012 Oct;10(10):1329-33. doi: 10.1586/erc.12.92. Expert Rev Cardiovasc Ther. 2012. PMID: 23190071 Review.
-
Toward "pain-free" statin prescribing: clinical algorithm for diagnosis and management of myalgia.Mayo Clin Proc. 2008 Jun;83(6):687-700. doi: 10.4065/83.6.687. Mayo Clin Proc. 2008. PMID: 18533086 Review.
Cited by
-
Discontinuation of statins in routine care settings: a cohort study.Ann Intern Med. 2013 Apr 2;158(7):526-34. doi: 10.7326/0003-4819-158-7-201304020-00004. Ann Intern Med. 2013. PMID: 23546564 Free PMC article.
-
Hyperlipidemia: An Evidence-based Review of Current Guidelines.Cureus. 2020 Mar 19;12(3):e7326. doi: 10.7759/cureus.7326. Cureus. 2020. PMID: 32313767 Free PMC article. Review.
-
Uncovering the Relationship Between Statins and Muscle Problems in the ELSA-Brasil MSK Cohort.Cardiovasc Drugs Ther. 2024 Dec;38(6):1409-1414. doi: 10.1007/s10557-023-07476-7. Epub 2023 Jun 1. Cardiovasc Drugs Ther. 2024. PMID: 37261675
-
Characterization of Statin-Associated Myopathy Case Reports in Thailand Using the Health Product Vigilance Center Database.Drug Saf. 2013 Sep;36(9):779-87. doi: 10.1007/s40264-013-0055-5. Drug Saf. 2013. PMID: 23615756
-
Fibromyalgia has a high prevalence and impact in cardiac failure patients.Eur J Rheumatol. 2017 Dec;4(4):245-249. doi: 10.5152/eurjrheum.2017.17026. Epub 2017 Nov 2. Eur J Rheumatol. 2017. PMID: 29308277 Free PMC article.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1001/jama.290.17.2243', 'is_inner': False, 'url': 'https://doi.org/10.1001/jama.290.17.2243'}, {'type': 'PubMed', 'value': '14600168', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14600168/'}]}
- Mitka M. Expanding statin use to help more at-risk patients is causing financial heartburn. JAMA. 2003;290(17):2243–5. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.jacc.2006.04.070', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.jacc.2006.04.070'}, {'type': 'PubMed', 'value': '16875966', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16875966/'}]}
- Cannon CP, Steinberg BA, Murphy SA, Mega JL, Braunwald E. Meta-analysis of cardiovascular outcomes trials comparing intensive versus moderate statin therapy. J Am Coll Cardiol. 2006;48(3):438–45. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0002-9149(03)00506-X', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0002-9149(03)00506-x'}, {'type': 'PubMed', 'value': '12867252', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12867252/'}]}
- Fonarow GC, Watson KE. Effective strategies for long-term statin use. Am J Cardiol. 2003;92(1A):27i–34i. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1007/s11883-002-0060-0', 'is_inner': False, 'url': 'https://doi.org/10.1007/s11883-002-0060-0'}, {'type': 'PubMed', 'value': '11772420', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11772420/'}]}
- Black DM. A general assessment of the safety of HMG CoA reductase inhibitors (statins). Curr Atheroscler Rep. 2002;4(1):34–41. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0002-9343(02)01428-6', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0002-9343(02)01428-6'}, {'type': 'PubMed', 'value': '12505120', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12505120/'}]}
- Sacks FM. Adherence to statin therapy: why aren’t we doing better? Am J Med. 2002;113(8):685–6. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
