

Empirically derived decision trees for the treatment of late-life depression
- PMID: 18450930
- PMCID: PMC2840395
- DOI: 10.1176/appi.ajp.2008.07081340
Empirically derived decision trees for the treatment of late-life depression
Abstract
Objective: Several predictors of treatment response in late-life depression have been reported in the literature. The aim of this analysis was to develop a clinically useful algorithm that would allow clinicians to predict which patients will likely respond to treatment and thereby guide clinical decision making.
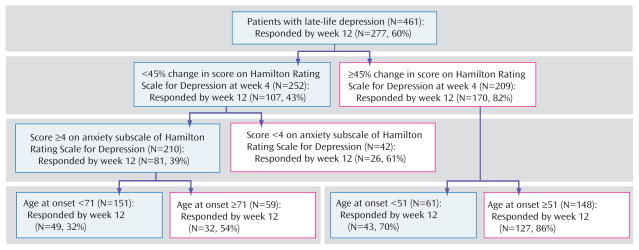
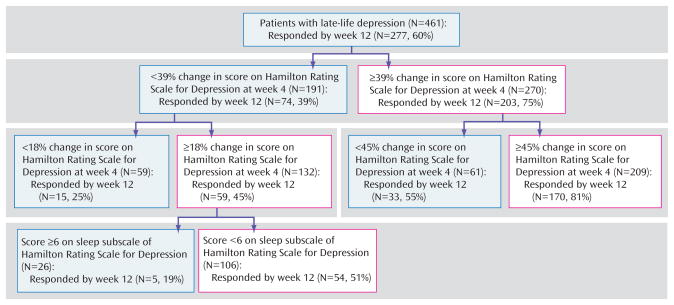
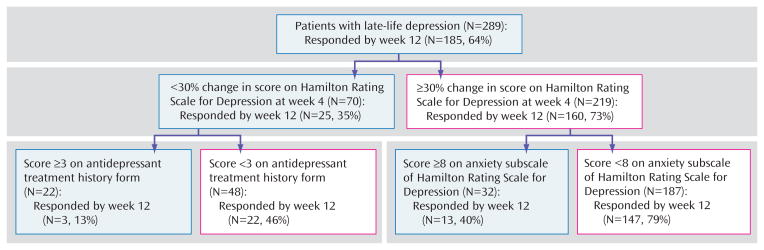
Method: A total of 461 patients with late-life depression were treated under structured conditions for up to 12 weeks and assessed weekly with the 17-item Hamilton Rating Scale for Depression (HAM-D-17). The authors developed a hierarchy of predictors of treatment response using signal-detection theory. The authors developed two models, one minimizing false predictions of future response and one minimizing false predictions of future nonresponse, to offer clinicians two clinically useful treatment algorithms.
Results: In the first model, early symptom improvement (defined by the relative change in HAM-D-17 total score from baseline to week 4), lower baseline anxiety, and an older age of onset predict response at 12 weeks. In the second model, early symptom improvement represents the principal guide in tailoring treatment, followed by baseline anxiety level, baseline sleep disturbance, and--for a minority of patients--the adequacy of previous antidepressant treatment.
Conclusions: Our two models, developed to help clinicians in different clinical circumstances, illustrate the possibility of tailoring the treatment of late-life depression based on clinical characteristics and confirm the importance of early observed changes in clinical status.
Figures
Comment in
-
Personalizing the care of geriatric depression.Am J Psychiatry. 2008 Jul;165(7):790-2. doi: 10.1176/appi.ajp.2008.08040461. Am J Psychiatry. 2008. PMID: 18593780 No abstract available.
References
-
- Charney DS, Reynolds CF, III, Lewis L, Lebowitz BD, Sunderland T, Alexopoulos GS, Blazer DG, Katz IR, Meyers BS, Arean PA, Borson S, Brown C, Bruce ML, Callahan CM, Charlson ME, Conwell Y, Cuthbert BN, Devanand DP, Gibson MJ, Gottlieb GL, Krishnan KR, Laden SK, Lyketsos CG, Mulsant BH, Niederehe G, Olin JT, Oslin DW, Pearson J, Persky T, Pollock BG, Raetzman S, Reynolds M, Salzman C, Schultz R, Schwenk TL, Scolnick E, Unutzer J, Weissman MM, Young RC. Depression and Bipolar Support Alliance: Depression and Bipolar Support Alliance consensus statement on the unmet needs in diagnosis and treatment of mood disorders in late life. Arch Gen Psychiatry. 2003;60:664–672. - PubMed
-
- Mulsant BH, Pollock BG. Treatment-resistant depression in late life. J Geriatr Psychiatry Neurol. 1998;11:186–193. - PubMed
-
- Mulsant BH, Whyte E, Lenze EJ, Lotrich F, Karp JF, Pollock BG, Reynolds CF., III Achieving long-term optimal outcomes in geriatric depression and anxiety. CNS Spectr. 2003;8(12 suppl 3):27–34. - PubMed
-
- Guscott R, Grof P. The clinical meaning of refractory depression: a review for the clinician. Am J Psychiatry. 1991;148:695–704. - PubMed
Publication types
MeSH terms
Grants and funding
- K24 MH069430/MH/NIMH NIH HHS/United States
- MH-71944/MH/NIMH NIH HHS/United States
- P30 MH071944/MH/NIMH NIH HHS/United States
- MH-69430/MH/NIMH NIH HHS/United States
- MH-52247/MH/NIMH NIH HHS/United States
- MH-37869/MH/NIMH NIH HHS/United States
- MH-65416/MH/NIMH NIH HHS/United States
- R01 MH037869/MH/NIMH NIH HHS/United States
- MH-43832/MH/NIMH NIH HHS/United States
- MH-30915/MH/NIMH NIH HHS/United States
- MH-067710/MH/NIMH NIH HHS/United States
- R01 MH043832/MH/NIMH NIH HHS/United States
- R37 MH043832/MH/NIMH NIH HHS/United States
- P30 MH052247/MH/NIMH NIH HHS/United States
- P30 MH030915/MH/NIMH NIH HHS/United States
- K23 MH067710/MH/NIMH NIH HHS/United States
- K24 MH065416/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
