

The relative timing of VMO and VL in the aetiology of anterior knee pain: a systematic review and meta-analysis
- PMID: 18452611
- PMCID: PMC2386790
- DOI: 10.1186/1471-2474-9-64
The relative timing of VMO and VL in the aetiology of anterior knee pain: a systematic review and meta-analysis
Abstract
Background: Anterior knee pain (AKP) is a common musculoskeletal complaint. It has been suggested that one factor that may contribute to the presence of AKP is a delay in the recruitment of the vastus medialis oblique muscle (VMO) relative to the vastus lateralis muscle (VL). There is however little consensus within the literature regarding the existence or nature of any such delay in the recruitment of the VMO within the AKP population. The purpose of this systematic review and meta-analysis was to examine the relative timing of onset of the VMO and VL in those with AKP in comparison to the asymptomatic population.
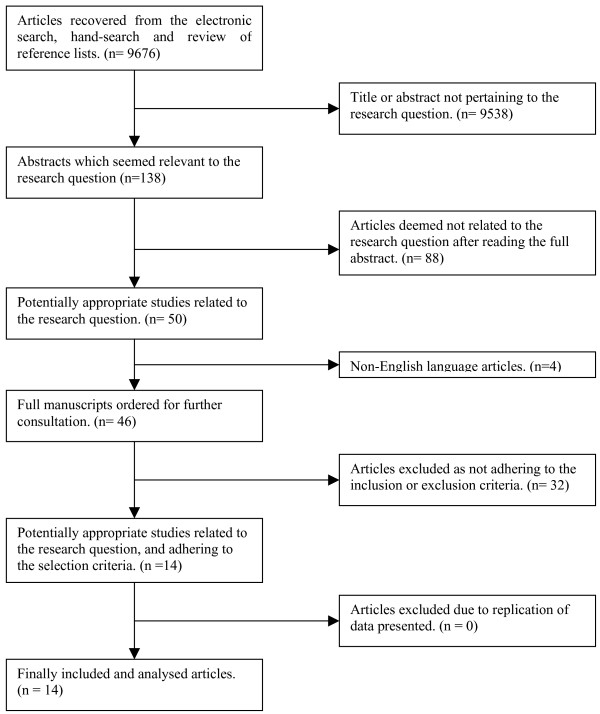
Methods: The bibliographic databases AMED, British Nursing Index, CINAHL, EMBASE, Ovid Medline, PEDro, Pubmed and the Cochrane Library were searched for studies comparing the timing of EMG onset of the VMO and VL in those with AKP versus the asymptomatic population. Studies fulfilling the inclusion criteria were independently assessed. Heterogeneity across the studies was measured. A meta-analysis of results was completed for those studies where adequate data was supplied. Where comparable methodologies had been used, results were pooled and analysed.
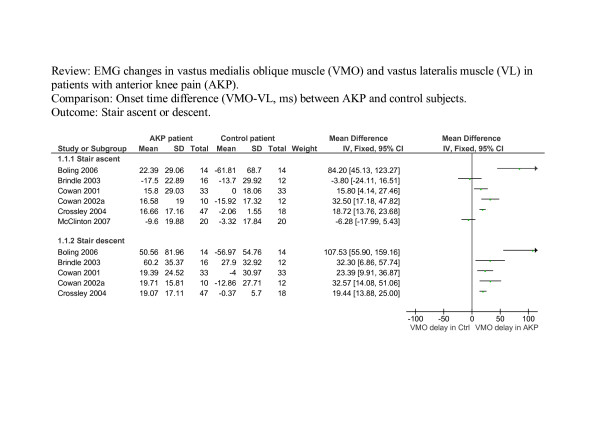
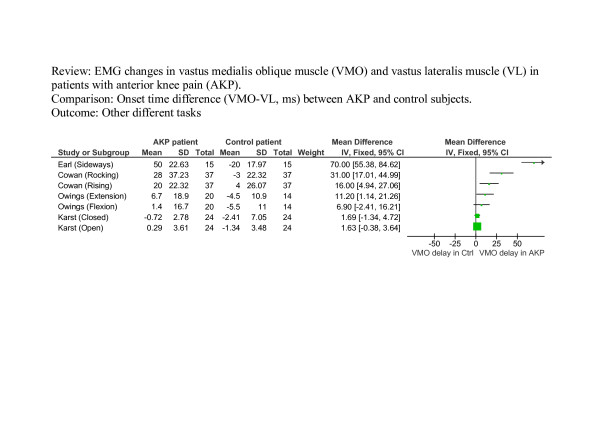
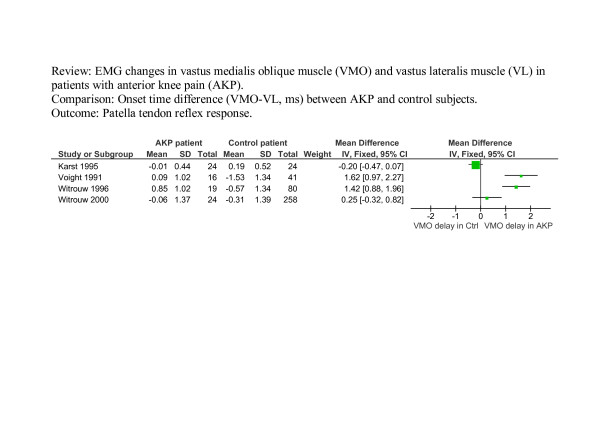
Results: Fourteen studies met the inclusion criteria; one prospective and thirteen observational case control. Eleven compared VMO and VL EMG onset times during voluntary active tasks while four investigated reflex response times. All used convenience sampling and did not state blinding of the assessor. Study methodologies/testing and assessment procedures varied and there was considerable heterogeneity within individual samples. Whilst a trend was identified towards a delay in onset of VMO relative to the VL in the AKP population during both voluntary active tasks and reflex activity, a substantial degree of heterogeneity across the pooled studies was identified (I2 = 69.9-93.4%, p < 0.01).
Conclusion: Findings are subject to substantial and unexplained heterogeneity. A trend was demonstrated towards a delayed onset of VMO relative to VL in those with AKP in comparison to those without. However not all AKP patients demonstrate a VMO-VL dysfunction, and this is compounded by normal physiological variability in the healthy population. The clinical and therapeutic significance is therefore difficult to assess.
Figures
Similar articles
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
The measurement and monitoring of surgical adverse events.Health Technol Assess. 2001;5(22):1-194. doi: 10.3310/hta5220. Health Technol Assess. 2001. PMID: 11532239
-
Eliciting adverse effects data from participants in clinical trials.Cochrane Database Syst Rev. 2018 Jan 16;1(1):MR000039. doi: 10.1002/14651858.MR000039.pub2. Cochrane Database Syst Rev. 2018. PMID: 29372930 Free PMC article.
Cited by
-
Influence of step rate and quadriceps load distribution on patellofemoral cartilage contact pressures during running.J Biomech. 2015 Aug 20;48(11):2871-8. doi: 10.1016/j.jbiomech.2015.04.036. Epub 2015 May 22. J Biomech. 2015. PMID: 26070646 Free PMC article.
-
Nature of the coupling between neural drive and force-generating capacity in the human quadriceps muscle.Proc Biol Sci. 2015 Nov 22;282(1819):20151908. doi: 10.1098/rspb.2015.1908. Proc Biol Sci. 2015. PMID: 26609085 Free PMC article.
-
Physical Therapist Management of Anterior Knee Pain.Curr Rev Musculoskelet Med. 2020 Dec;13(6):776-787. doi: 10.1007/s12178-020-09678-0. Epub 2020 Oct 30. Curr Rev Musculoskelet Med. 2020. PMID: 33128200 Free PMC article. Review.
-
PAIN, FUNCTION, AND STRENGTH OUTCOMES FOR MALES AND FEMALES WITH PATELLOFEMORAL PAIN WHO PARTICIPATE IN EITHER A HIP/CORE- OR KNEE-BASED REHABILITATION PROGRAM.Int J Sports Phys Ther. 2016 Dec;11(6):926-935. Int J Sports Phys Ther. 2016. PMID: 27904794 Free PMC article.
-
Diagnostic algorithm in aseptic TKA failure - What is evidence-based?J Orthop. 2021 Mar 21;24:248-253. doi: 10.1016/j.jor.2021.03.006. eCollection 2021 Mar-Apr. J Orthop. 2021. PMID: 33854292 Free PMC article. No abstract available.
References
-
- McConnell J. The management of chondromalacia patellae: a long term solution. Aust J Physiother. 1986;32:215–223. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
