

Kindler syndrome and periodontal disease: review of the literature and a 12-year follow-up case
- PMID: 18454678
- PMCID: PMC2697853
- DOI: 10.1902/jop.2008.070167
Kindler syndrome and periodontal disease: review of the literature and a 12-year follow-up case
Abstract
Background: The association of aggressive periodontitis with Kindler syndrome was based on a single case in 1996 and later confirmed with a larger population. Since then, significant research has greatly increased our understanding of the molecular pathology of this disorder. We review recent advances in the molecular mechanisms of the syndrome and present a maintenance case report of a patient who has been followed in our clinic.
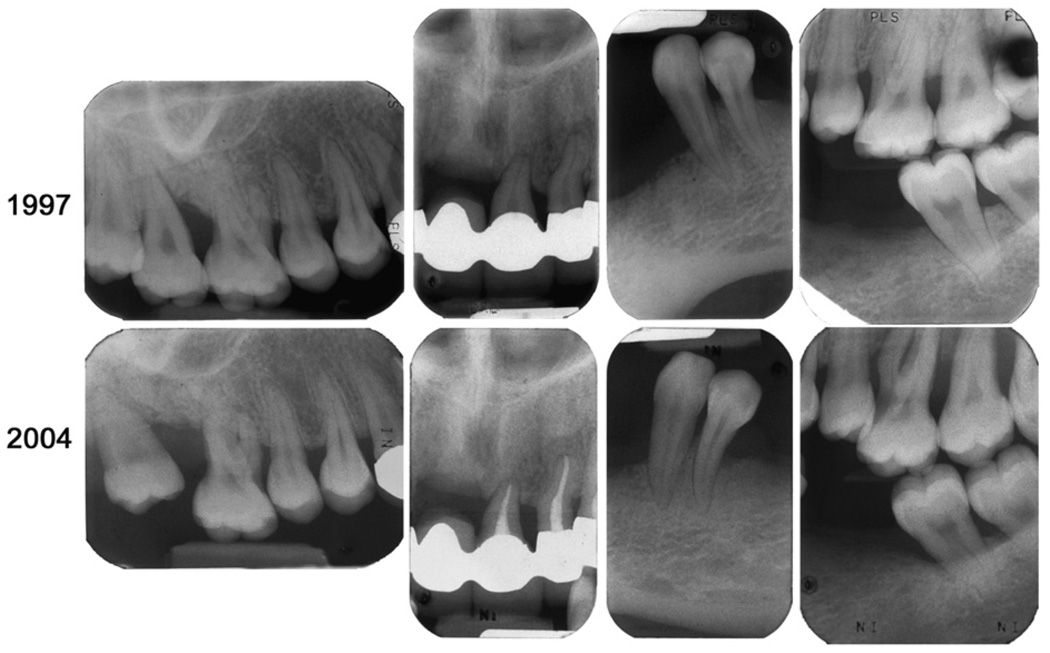
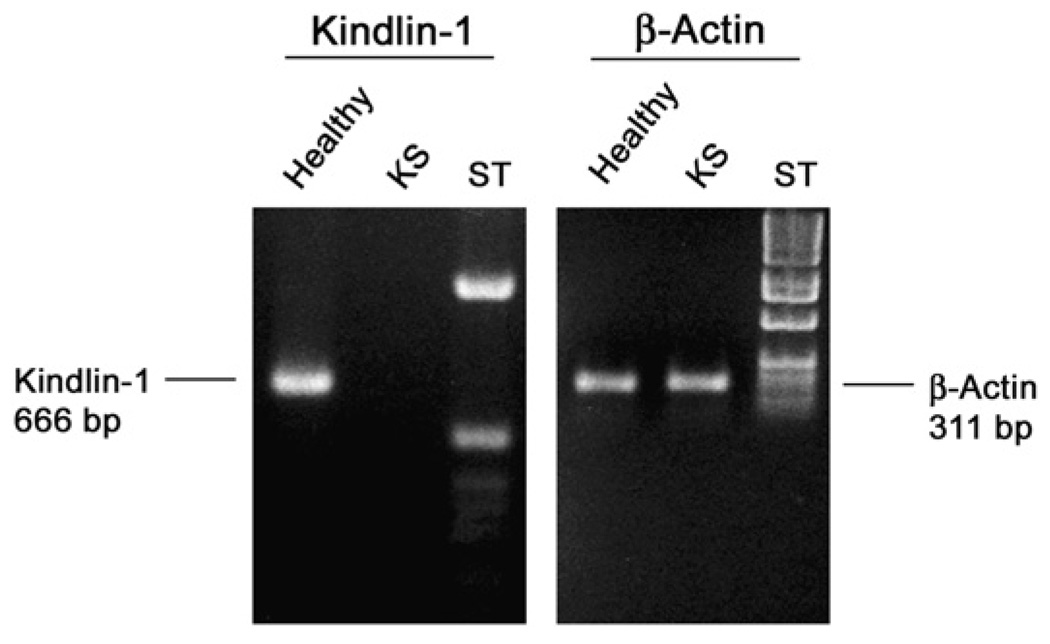
Methods: A female patient who was diagnosed with Kindler syndrome and aggressive periodontitis at the age of 16 years has been followed and treated in our clinic for 12 years. Her main treatment has been maintenance therapy following her initial treatment and restorative work previously documented. Gingival biopsies obtained during the recent extraction of hopeless maxillary molars were used for histologic assessment of gingival tissue attachment apparatus and to isolate gingival fibroblasts. Reverse transcription-polymerase chain reaction (RT-PCR) was performed using these cells to confirm the lack of expression of kindlin-1.
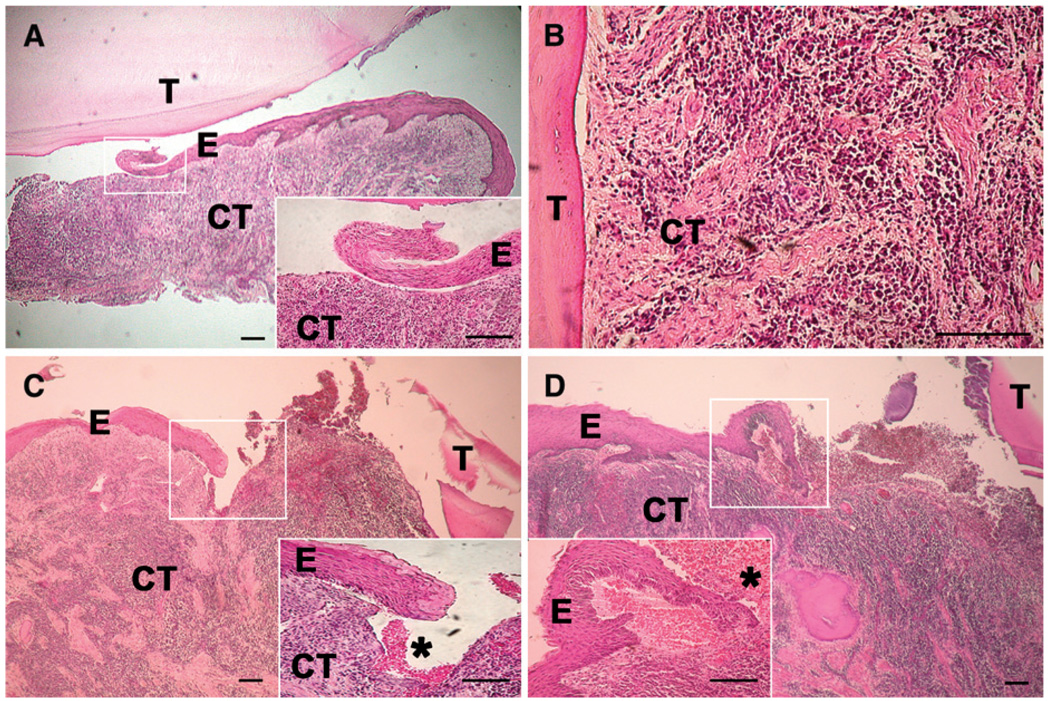
Results: RT-PCR showed the total loss of kindlin-1 mRNA in cultured gingival fibroblasts, supporting the clinical diagnosis of Kindler syndrome. Tissue biopsies revealed atypical pocket epithelium. Maintenance therapy has been moderately successful. Teeth that were recently lost had a poor prognosis at the initial assessment. The patient's gingiva and oral mucosa continue to be fragile with episodes of sloughing and inflammation.
Conclusions: Periodontitis in Kindler syndrome responds to maintenance therapy, but the gingiva and oral mucosa continue to display an abnormal appearance with white patches. Histologic findings suggest that the junctional epithelium in Kindler syndrome may be abnormal and could explain why these patients have periodontal disease. Attachment loss progressed around teeth with an initial guarded or poor prognosis. Teeth that started with a good or fair prognosis continue to have a fair prognosis. Limited dental implant treatment is being considered.
Figures

References
-
- Wiebe CB, Silver JG, Larjava HS. Early-onset periodontitis associated with Weary-Kindler syndrome. J Periodontol. 1996;67:1004–1010. - PubMed
-
- Wiebe CB, Penagos H, Luong N, et al. Clinical and microbiologic study of periodontitis associated with Kindler syndrome. J Periodontol. 2003;74:25–31. - PubMed
-
- Kindler T. Congenital poikiloderma with traumatic bulla formation and progressive cutaneous atrophy. Br J Dermatol. 1954;66:104–111. - PubMed
-
- Patrizi A, Pauluzzi P, Neri I, Trevisan G, De Giorgi LB, Pasquinelli G. Kindler syndrome: Report of a case with ultrastructural study and review of the literature. Pediatr Dermatol. 1996;13:397–402. - PubMed
-
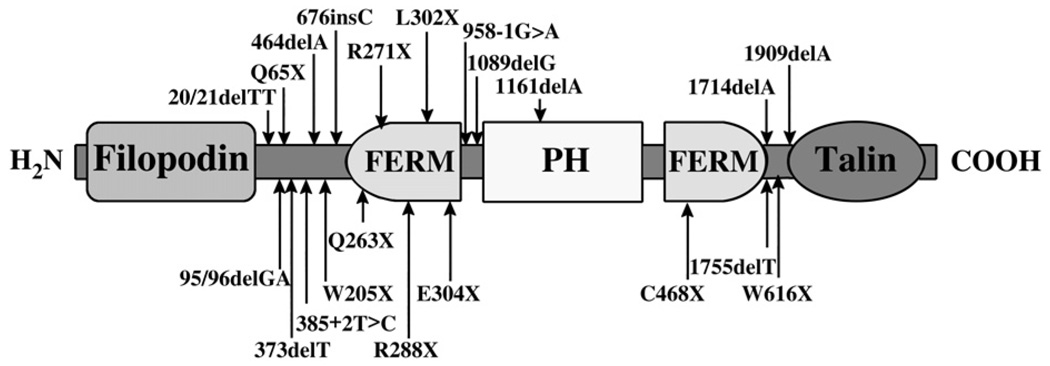
- Jobard F, Bouadjar B, Caux F, et al. Identification of mutations in a new gene encoding a FERM family protein with a pleckstrin homology domain in Kindler syndrome. Hum Mol Genet. 2003;12:925–935. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
