

Antimicrobial treatment for ventilator-associated tracheobronchitis: a randomized, controlled, multicenter study
- PMID: 18454864
- PMCID: PMC2481443
- DOI: 10.1186/cc6890
Antimicrobial treatment for ventilator-associated tracheobronchitis: a randomized, controlled, multicenter study
Abstract
Introduction: Ventilator-associated tracheobronchitis (VAT) is associated with increased duration of mechanical ventilation. We hypothesized that, in patients with VAT, antibiotic treatment would be associated with reduced duration of mechanical ventilation.
Methods: We conducted a prospective, randomized, controlled, unblinded, multicenter study. Patients were randomly assigned (1:1) to receive or not receive intravenous antibiotics for 8 days. Patients with ventilator-associated pneumonia (VAP) prior to VAT and those with severe immunosuppression were not eligible. The trial was stopped early because a planned interim analysis found a significant difference in intensive care unit (ICU) mortality.
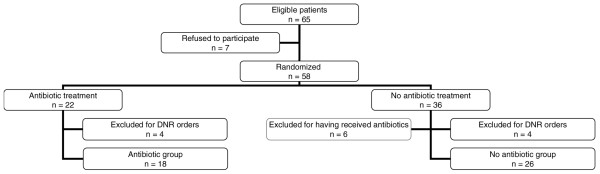
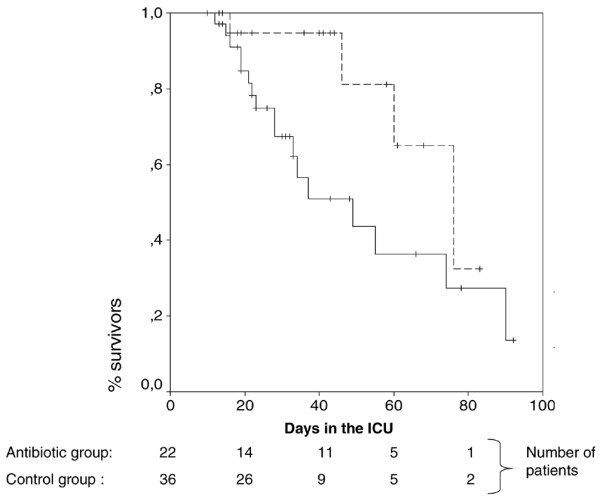
Results: Fifty-eight patients were randomly assigned. Patient characteristics were similar in the antibiotic (n = 22) and no antibiotic (n = 36) groups. Pseudomonas aeruginosa was identified in 32% of VAT episodes. Although no difference was found in mechanical ventilation duration and length of ICU stay, mechanical ventilation-free days were significantly higher (median [interquartile range], 12 [8 to 24] versus 2 [0 to 6] days, P < 0.001) in the antibiotic group than in the no antibiotic group. In addition, subsequent VAP (13% versus 47%, P = 0.011, odds ratio [OR] 0.17, 95% confidence interval [CI] 0.04 to 0.70) and ICU mortality (18% versus 47%, P = 0.047, OR 0.24, 95% CI 0.07 to 0.88) rates were significantly lower in the antibiotic group than in the no antibiotic group. Similar results were found after exclusion of patients with do-not-resuscitate orders and those randomly assigned to the no antibiotic group but who received antibiotics for infections other than VAT or subsequent VAP.
Conclusion: In patients with VAT, antimicrobial treatment is associated with a greater number of days free of mechanical ventilation and lower rates of VAP and ICU mortality. However, antibiotic treatment has no significant impact on total duration of mechanical ventilation.
Trial registration: ClinicalTrials.gov, number NCT00122057.
Figures
Comment in
-
Ventilator-associated tracheobronchitis (VAT): questions, answers, and a new paradigm?Crit Care. 2008;12(3):157. doi: 10.1186/cc6912. Epub 2008 Jun 18. Crit Care. 2008. PMID: 18598373 Free PMC article.
-
Ventilator-associated tracheobronchitis: where are we now?Rev Bras Ter Intensiva. 2014 Jul-Sep;26(3):212-4. doi: 10.5935/0103-507x.20140033. Rev Bras Ter Intensiva. 2014. PMID: 25295816 Free PMC article. No abstract available.
References
-
- Nseir S, Di Pompeo C, Pronnier P, Beague S, Onimus T, Saulnier F, Grandbastien B, Mathieu D, Delvallez-Roussel M, Durocher A. Nosocomial tracheobronchitis in mechanically ventilated patients: incidence, aetiology and outcome. Eur Respir J. 2002;20:1483–1489. doi: 10.1183/09031936.02.00012902. - DOI - PubMed
-
- Bouza E, Pérez A, Muñoz P, Jesús Pérez M, Rincón C, Sánchez C, Martín-Rabadán P, Riesgo M, Cardiovascular Infection Study Group Ventilator-associated pneumonia after heart surgery: a prospective analysis and the value of surveillance. Crit Care Med. 2003;31:1964–1970. doi: 10.1097/01.ccm.0000084807.15352.93. - DOI - PubMed
-
- Nseir S, Di Pompeo C, Soubrier S, Lenci H, Delour P, Onimus T, Saulnier F, Mathieu D, Durocher A. Effect of ventilator-associated tracheobronchitis on outcome in patients without chronic respiratory failure: a case-control study. Crit Care. 2005;9:R238–R245. doi: 10.1186/cc3508. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
