

Beam path toxicities to non-target structures during intensity-modulated radiation therapy for head and neck cancer
- PMID: 18455324
- PMCID: PMC9627578
- DOI: 10.1016/j.ijrobp.2008.01.012
Beam path toxicities to non-target structures during intensity-modulated radiation therapy for head and neck cancer
Abstract
Background: Intensity-modulated radiation therapy (IMRT) beams traverse nontarget normal structures not irradiated during three-dimensional conformal RT (3D-CRT) for head and neck cancer (HNC). This study estimates the doses and toxicities to nontarget structures during IMRT.
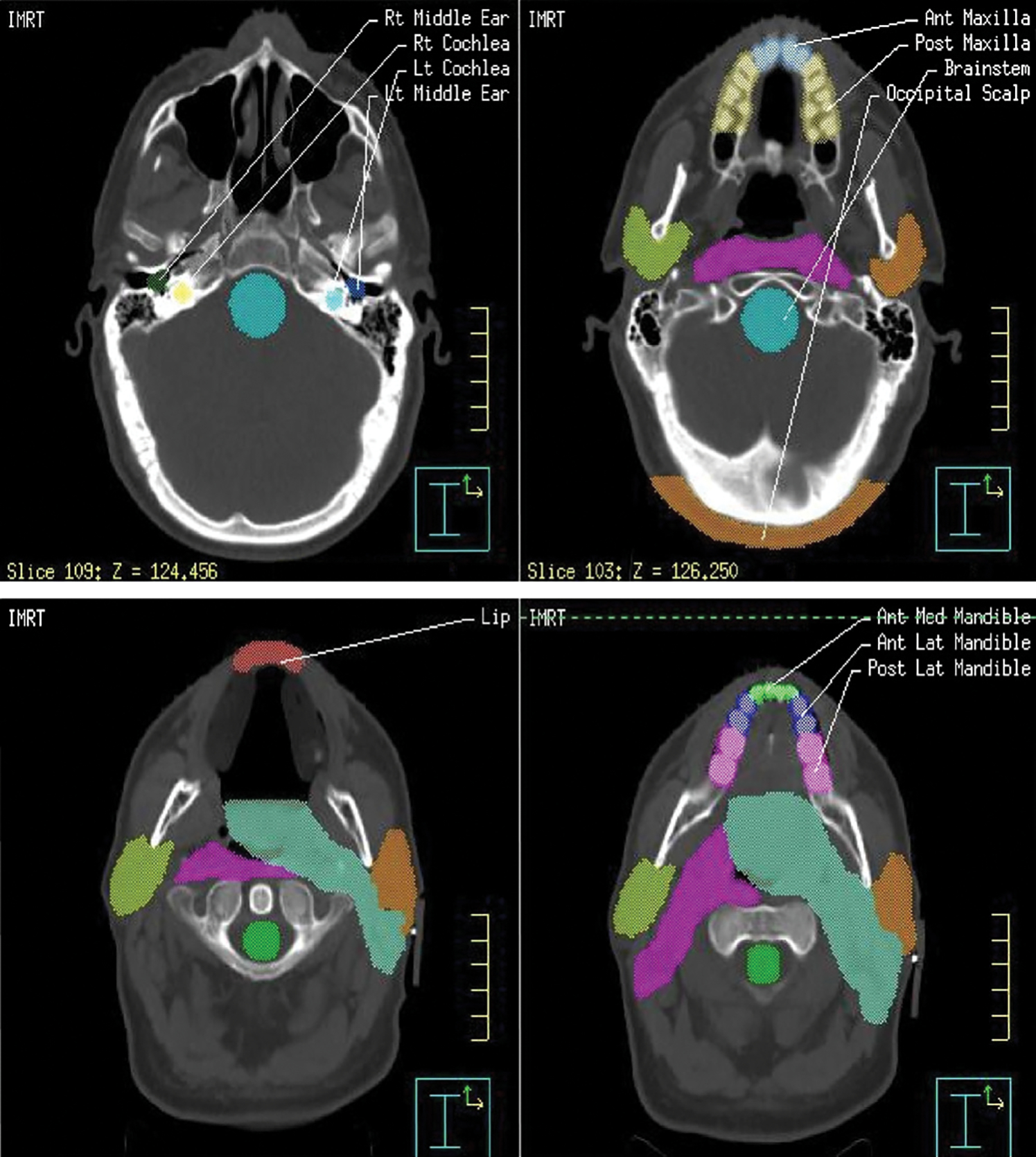
Materials and methods: Oropharyngeal cancer IMRT and 3D-CRT cases were reviewed. Dose-volume histograms (DVH) were used to evaluate radiation dose to the lip, cochlea, brainstem, occipital scalp, and segments of the mandible. Toxicity rates were compared for 3D-CRT, IMRT alone, or IMRT with concurrent cisplatin. Descriptive statistics and exploratory recursive partitioning analysis were used to estimate dose "breakpoints" associated with observed toxicities.
Results: A total of 160 patients were evaluated for toxicity; 60 had detailed DVH evaluation and 15 had 3D-CRT plan comparison. Comparing IMRT with 3D-CRT, there was significant (p </= 0.002) nonparametric differential dose to all clinically significant structures of interest. Thirty percent of IMRT patients had headaches and 40% had occipital scalp alopecia. A total of 76% and 38% of patients treated with IMRT alone had nausea and vomiting, compared with 99% and 68%, respectively, of those with concurrent cisplatin. IMRT had a markedly distinct toxicity profile than 3D-CRT. In recursive partitioning analysis, National Cancer Institute's Common Toxicity Criteria adverse effects 3.0 nausea and vomiting, scalp alopecia and anterior mucositis were associated with reconstructed mean brainstem dose >36 Gy, occipital scalp dose >30 Gy, and anterior mandible dose >34 Gy, respectively.
Conclusions: Dose reduction to specified structures during IMRT implies an increased beam path dose to alternate nontarget structures that may result in clinical toxicities that were uncommon with previous, less conformal approaches. These findings have implications for IMRT treatment planning and research, toxicity assessment, and multidisciplinary patient management.
Conflict of interest statement
Conflict of interest: none.
Figures



References
-
- Mohan R, Wu Q, Manning M, et al. Radiobiological considerations in the design of fractionation strategies for intensity-modulated radiation therapy of head and neck cancers. Int J Radiat Oncol Biol Phys 2000;46:619–630. - PubMed
-
- Mell LK, Mehrotra AK, Mundt AJ. Intensity-modulated radiation therapy use in the US, 2004. Cancer 2005;104:1296–1303. - PubMed
-
- Radiation-induced emesis: A prospective observational multi-center Italian trial. The Italian Group for Antiemetic Research in Radiotherapy. Int J Radiat Oncol Biol Phys 1999;44:619–625. - PubMed
-
- Kris MG, Hesketh PJ, Somerfield MR, et al. American Society of Clinical Oncology Guideline for Antiemetics in Oncology: Update 2006. J Clin Oncol 2006;24:2932–2947. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
