

Characterization of ultrasound propagation through ex-vivo human temporal bone
- PMID: 18456391
- PMCID: PMC4921610
- DOI: 10.1016/j.ultrasmedbio.2008.02.012
Characterization of ultrasound propagation through ex-vivo human temporal bone
Abstract
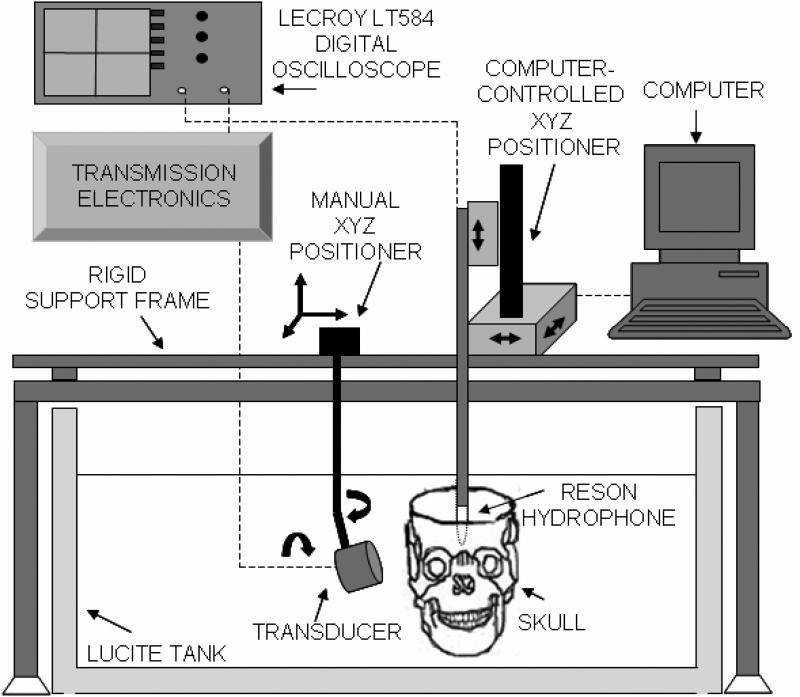
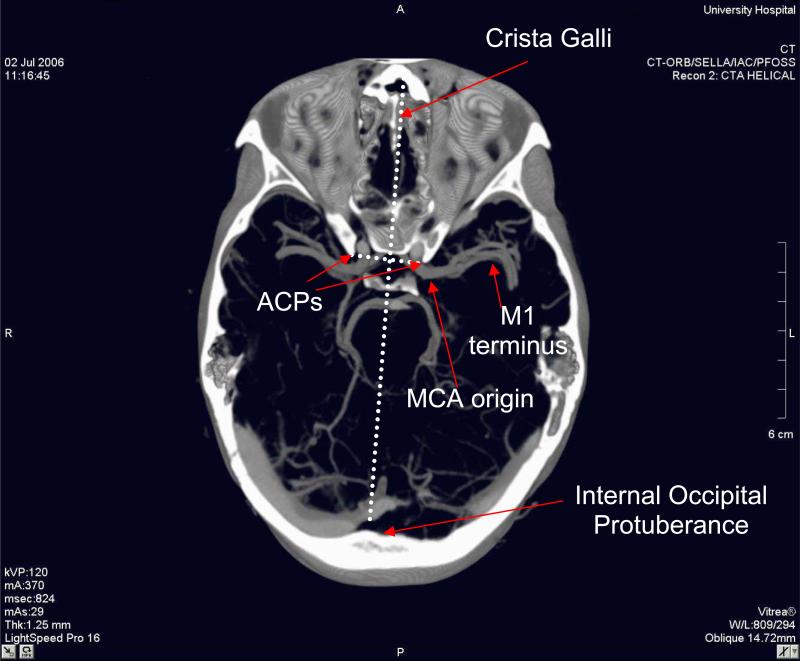
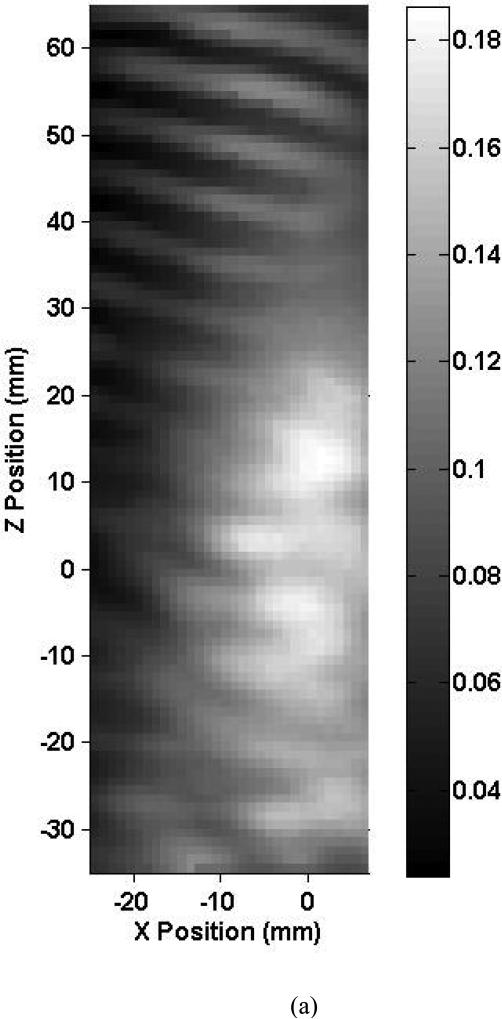
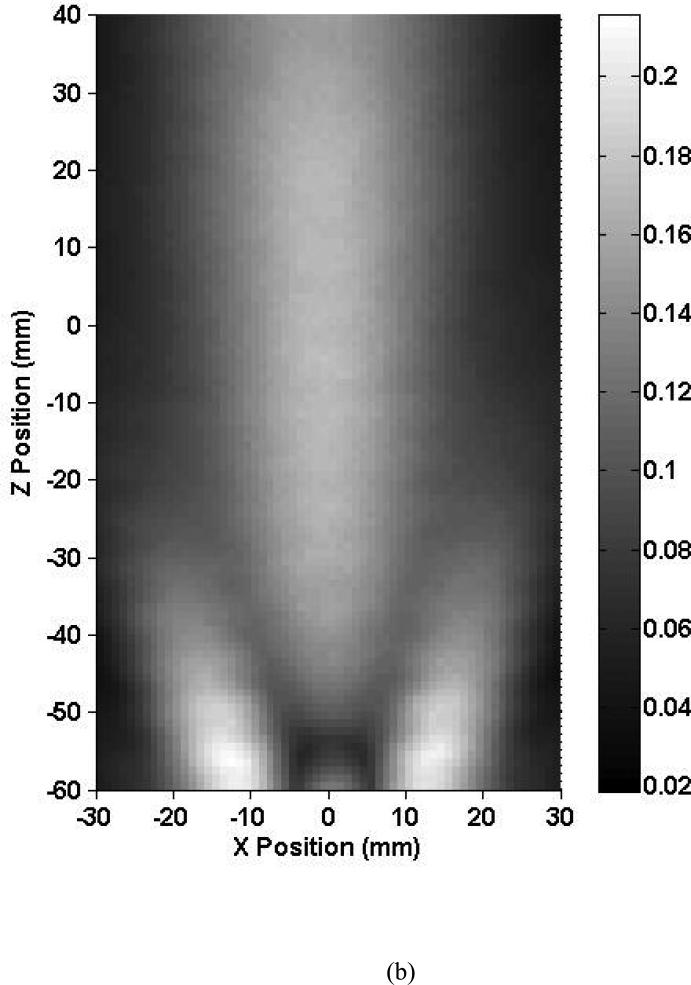
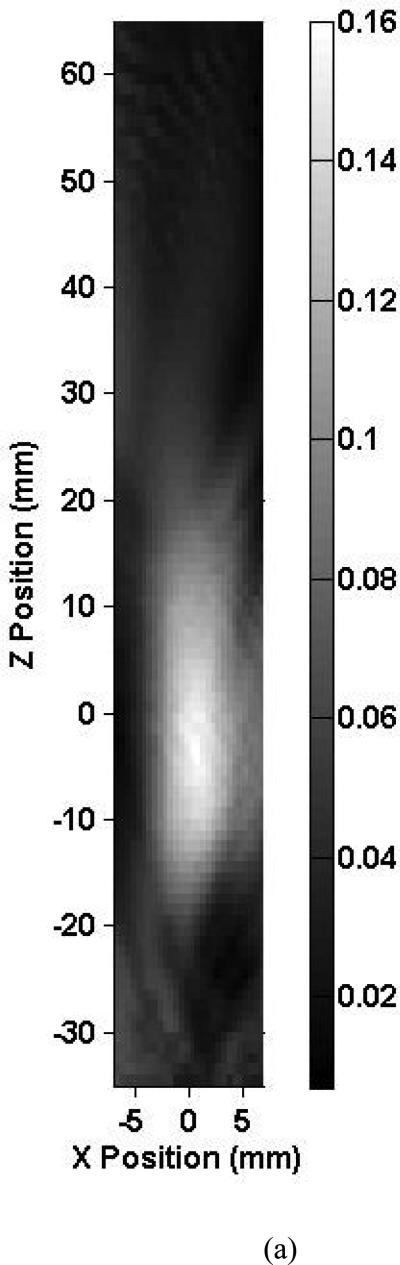
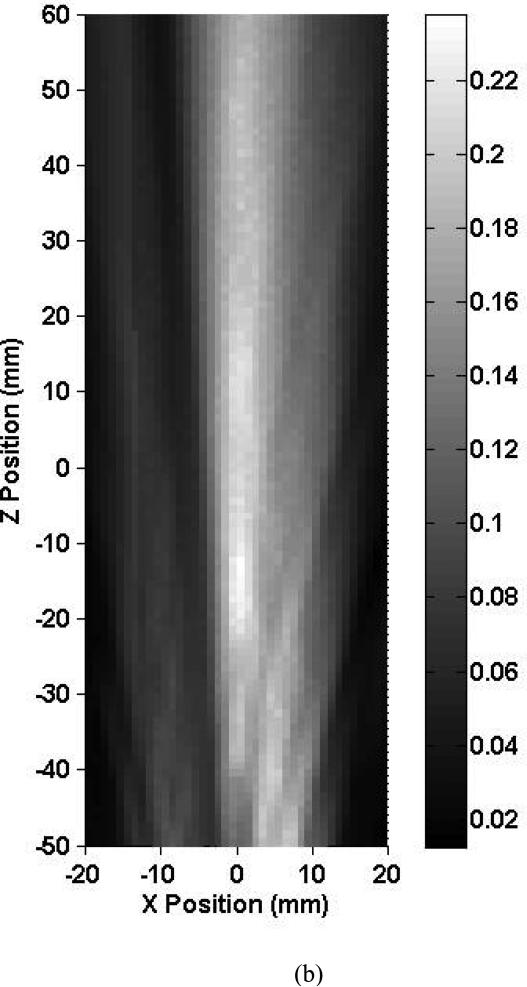
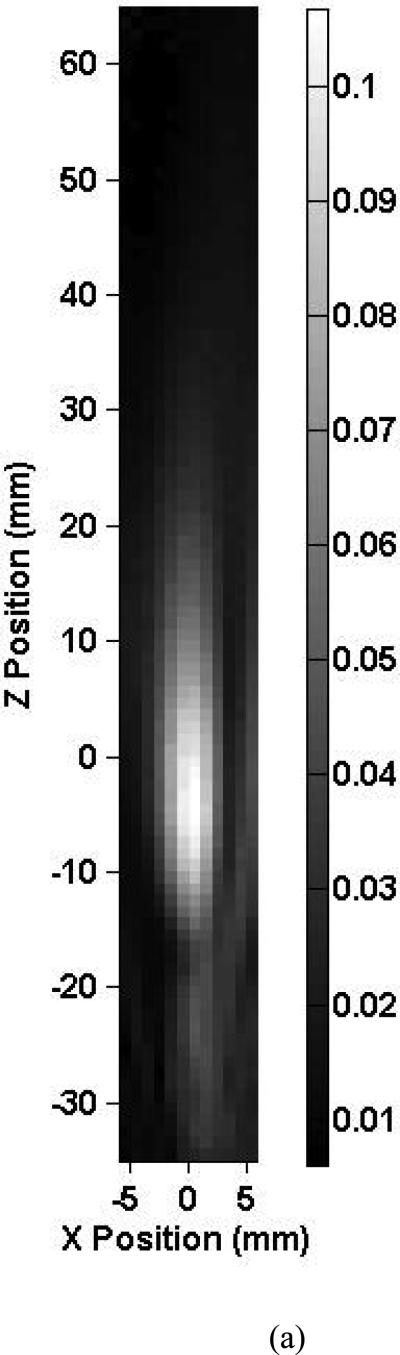
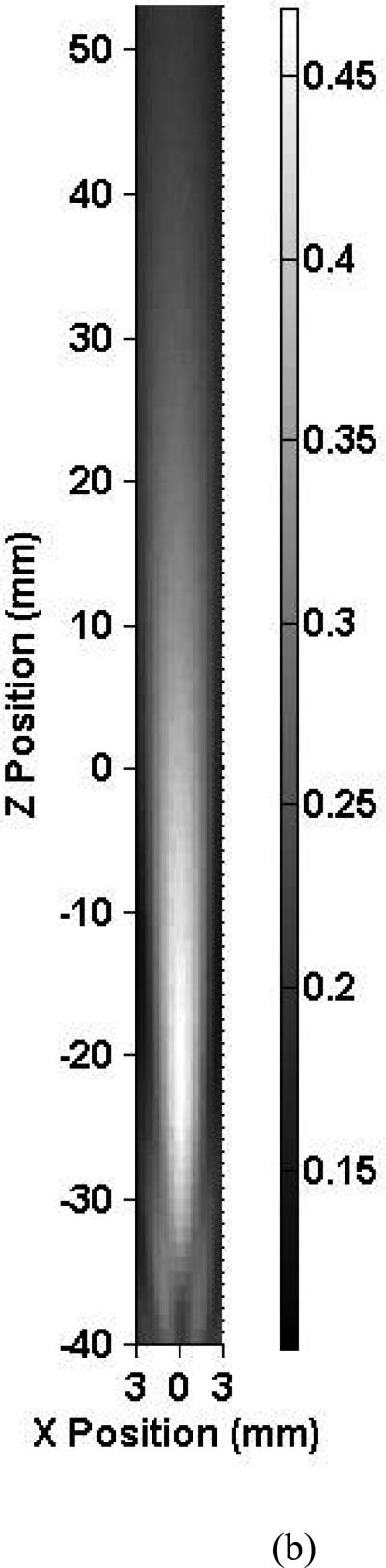
Adjuvant therapies that lower the thrombolytic dose or increase its efficacy would represent a significant breakthrough in the treatment of patients with ischemic stroke. The objective of this study was to perform intracranial measurements of the acoustic pressure field generated by 0.12, 1.03 and 2.00-MHz ultrasound transducers to identify optimal ultrasound parameters that would maximize penetration and minimize aberration of the beam. To achieve this goal, in vitro experiments were conducted on five human skull specimens. In a water-filled tank, two unfocused transducers (0.12 and 1.03 MHz) and one focused transducer (2.00 MHz) were consecutively placed near the right temporal bone of each skull. A hydrophone, mounted on a micropositioning system, was moved to an estimated location of the middle cerebral artery (MCA) origin, and measurements of the surrounding acoustic pressure field were performed. For each measurement, the distance from the position of maximum acoustic pressure to the estimated origin of the MCA inside the skulls was quantified. The -3 dB depth-of-field and beamwidth in the skull were also investigated as a function of the three frequencies. Results show that the transducer alignment relative to the skull is a significant determinant of the detailed behavior of the acoustic field inside the skull. For optimal penetration, insonation normal to the temporal bone was needed. The shape of the 0.12-MHz intracranial beam was more distorted than those at 1.03 and 2.00 MHz because of the large aperture and beamwidth. However, lower ultrasound pressure reduction was observed at 0.12 MHz (22.5%). At 1.03 and 2.00 MHz, two skulls had an insufficient temporal bone window and attenuated the beam severely (up to 96.6% pressure reduction). For all frequencies, constructive and destructive interference patterns were seen near the contralateral skull wall at various elevations. The 0.12-MHz ultrasound beam depth-of-field was affected the most when passing through the temporal bone and showed a decrease in size of more than 55% on average. The speed of sound in the temporal bone of each skull was estimated at 1.03 MHz and demonstrated a large range (1752.1 to 3285.3 m/s). Attenuation coefficients at 1.03 and 2.00 MHz were also derived for each of the five skull specimens. This work provides needed information on ultrasound beam shapes inside the human skull, which is a necessary first step for the development of an optimal transcranial ultrasound-enhanced thrombolysis device.
Figures
References
-
- Ackerman LV, Buke MW, Boulos RS, Patel S. Computed measurements on computed tomograms of the head. Radiology. 1982;143:115–120. - PubMed
-
- Alexandrov AV, Molina CA, Grotta JC, Garami Z, Ford SR, Alvarez-Sabin J, Montaner J, Saqqur M, Demchuk AM, Moye LA, Hill MD, Wojner AW. Ultrasound-enhanced systemic thrombolysis for acute ischemic stroke. N Engl J Med. 2004;351:2170–8. - PubMed
-
- Azuma T, Kawabata K, Umemura S, Ogihara M, Kubota J, Sasaki A, Furuhata H. Bubble generaion by standing wave surrounding by cranium with transcranial ultrasound beam. Japanese Journalof Applied Physics. 2005;44:4625–4630.
-
- Berg-Dammer E, Mobius E, Nahser HC, Kuhne D. Local thrombolytic therapy for thromboembolic occlusion of the middle cerebral artery. Neurol Res. 1992;14:164–6. - PubMed
-
- Bruno A, Biller J, Silvidi JA. A reason for failure to obtain transcranial Doppler flow signals. Hyperostosis of the skull. Stroke. 1988;19:274. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
