

Prospective study of motor, sensory, psychologic, and autonomic functions in patients with irritable bowel syndrome
- PMID: 18456567
- PMCID: PMC2495078
- DOI: 10.1016/j.cgh.2008.02.060
Prospective study of motor, sensory, psychologic, and autonomic functions in patients with irritable bowel syndrome
Abstract
Background & aims: The aim of this study was to assess pathophysiology in irritable bowel syndrome (IBS).
Methods: A total of 122 IBS patients (3 male) and 41 healthy females underwent the following: questionnaires (symptoms, psychology), autonomic function, gut transit, gastric volumes, satiation, rectal compliance, and sensation (thresholds and pain ratings) testing. Proportions of patients with abnormal (<10th and >90th percentiles) motor or sensory functions according to bowel symptoms (constipation [C], diarrhea [D], mixed [M),) pain/bloat, and number of primary symptoms were estimated.
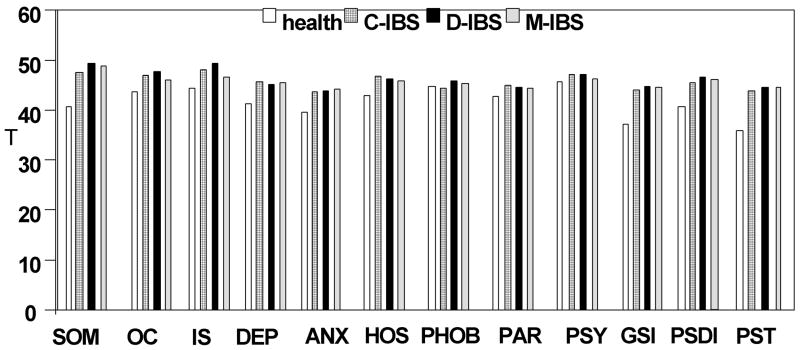
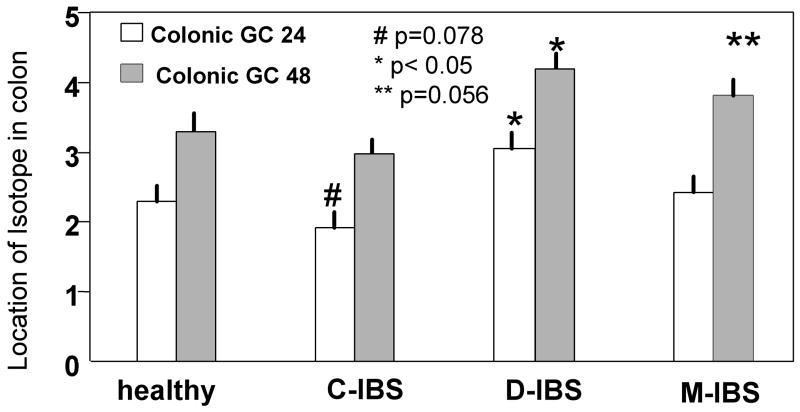
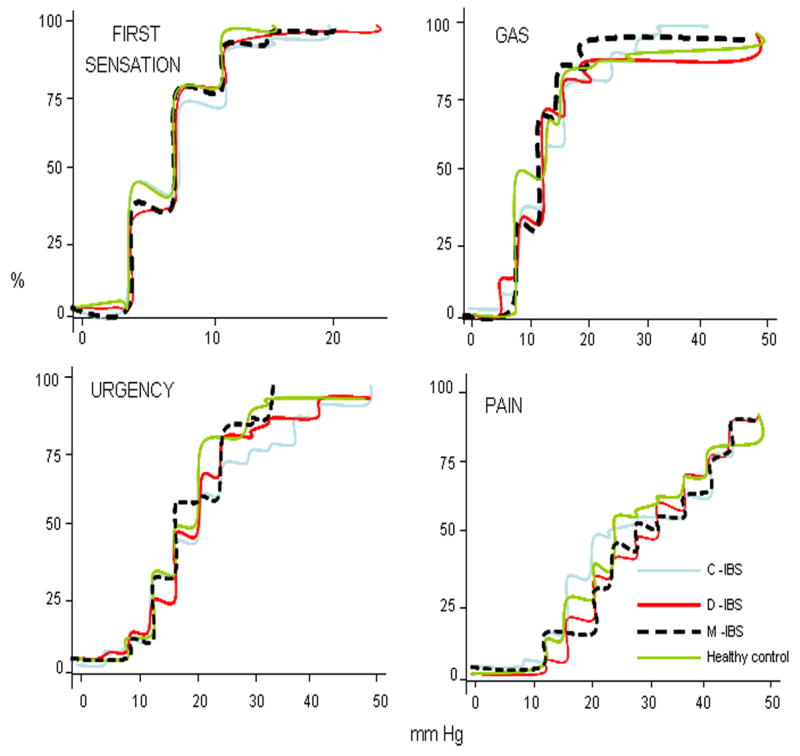
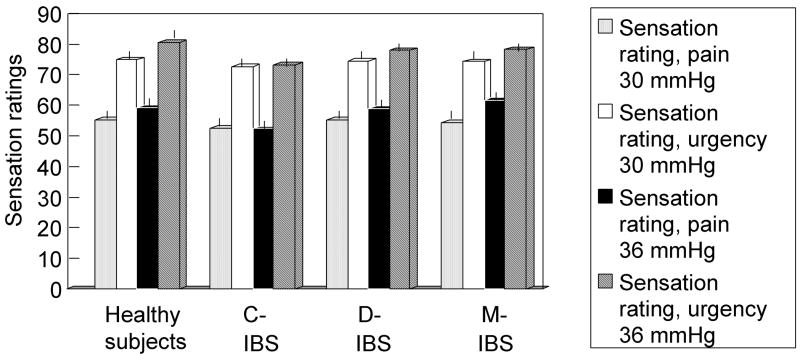
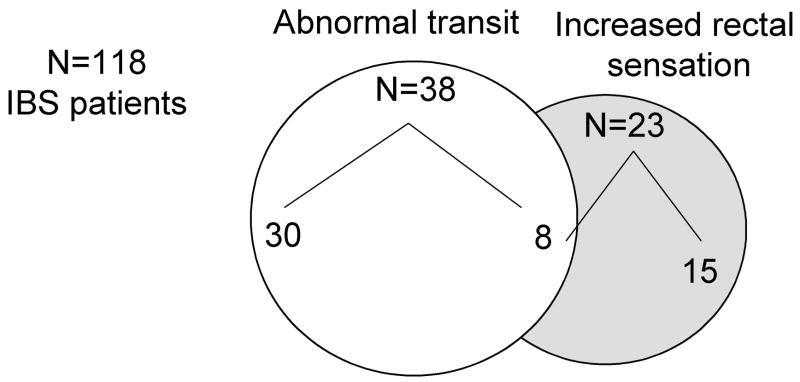
Results: IBS subgroups (C, D, M) were similar in age, gastric and small-bowel transit, satiation, gastric volumes, rectal compliance, sensory thresholds, and pain ratings. IBS was associated with body mass index, somatic symptoms, and anxiety and depression scores. Significant associations were observed with colonic transit (IBS-C [P = .078] and IBS-D [P < .05] at 24 h; IBS-D [P < .01] and IBS-M [P = .056] at 48 h): 32% of IBS patients had abnormal colonic transit: 20.5% at 24 hours and 11.5% at 48 hours. Overall, 20.5% of IBS patients had increased sensation to distensions: hypersensitivity (<10th percentile thresholds) in 7.6%, and hyperalgesia (pain sensation ratings to distension >90th percentile for ratings in health) in 13%. Conversely, 16.5% of IBS patients had reduced rectal sensation. Pain greater than 6 times per year and bloating were not associated significantly with motor, satiation, or sensory functions. Endorsing 1 to 2 or 3 to 4 primary IBS symptoms were associated with abnormal transit and sensation in IBS.
Conclusions: In tertiary referral (predominantly female) patients with IBS, colonic transit (32%) is the most prevalent physiologic abnormality; 21% had increased and 17% had decreased rectal pain sensations. Comprehensive physiologic assessment may help optimize management in IBS.
Conflict of interest statement
Disclosures: The authors have no conflicts of interest to disclose.
Figures
References
-
- Camilleri M. Mechanisms in IBS: something old, something new, something borrowed. Neurogastroenterol Motil. 2005;17:311–316. - PubMed
-
- Vassallo M, Camilleri M, Phillips SF, Brown ML, Chapman NJ, Thomforde GM. Transit through the proximal colon influences stool weight in the irritable bowel syndrome. Gastroenterology. 1992;102:102–108. - PubMed
-
- Stivland T, Camilleri M, Vassallo M, Proano M, Rath D, Brown M, Thomforde G, Pemberton J, Phillips S. Scintigraphic measurement of regional gut transit in idiopathic constipation. Gastroenterology. 1991;101:107–115. - PubMed
-
- Choi MG, Camilleri M, O’Brien MD, Kammer PP, Hanson RB. A pilot study of motility and tone of the left colon in patients with diarrhea due to functional disorders and dysautonomia. Am J Gastroenterol. 1997;92:297–302. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
