

Functionally distinct sodium channels in ventricular epicardial and endocardial cells contribute to a greater sensitivity of the epicardium to electrical depression
- PMID: 18456729
- PMCID: PMC2494739
- DOI: 10.1152/ajpheart.01327.2007
Functionally distinct sodium channels in ventricular epicardial and endocardial cells contribute to a greater sensitivity of the epicardium to electrical depression
Abstract
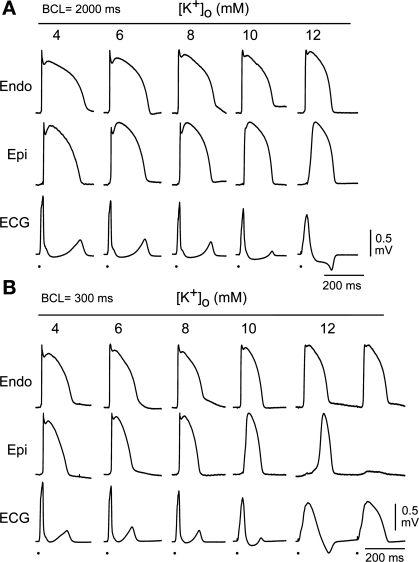
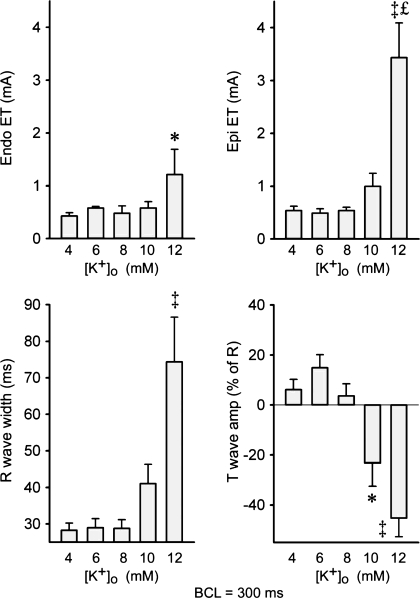
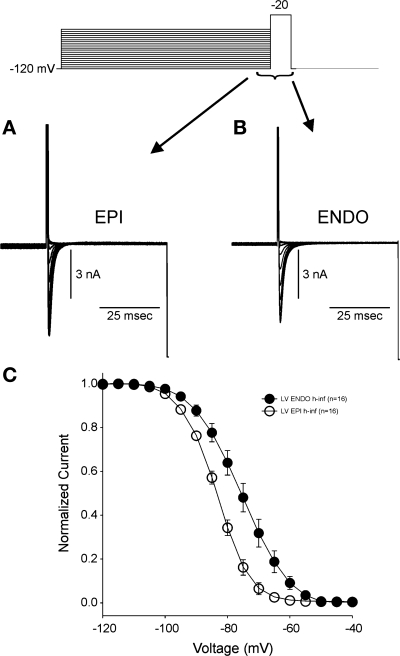
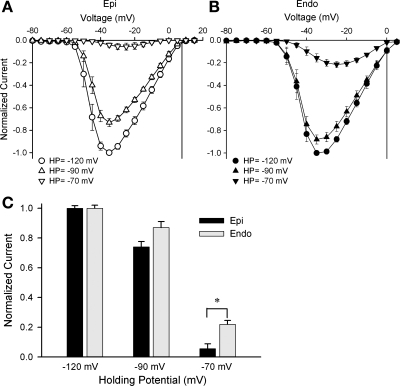
A greater depression of the action potential (AP) of the ventricular epicardium (Epi) versus endocardium (Endo) is readily observed in experimental models of acute ischemia and Brugada syndrome. Endo and Epi differences in transient outward K(+) current and/or ATP-sensitive K(+) channel current are believed to contribute to the differential response. The present study tested the hypothesis that the greater sensitivity of Epi is due in part to its functionally distinct early fast Na(+) current (I(Na)). APs were recorded from isolated Epi and Endo tissue slices and coronary-perfused wedge preparations before and after exposures to elevated extracellular K(+) concentration ([K(+)](o); 6-12 mM). I(Na) was recorded from Epi and Endo myocytes using whole cell patch-clamp techniques. In tissue slices, increasing [K(+)](o) to 12 mM reduced V(max) to 51.1 +/- 5.3% and 26.8 +/- 9.6% of control in Endo (n = 9) and Epi (n = 14), respectively (P < 0.05). In wedge preparations (n = 12), the increase in [K(+)](o) caused selective depression of Epi APs and transmural conduction slowing and block. I(Na) density was not significantly different between Epi (n = 14) and Endo (n = 15) cells, but Epi cells displayed a more negative half-inactivation voltage [-83.6 +/- 0.1 and -75.5 +/- 0.3 mV for Epi (n = 16) and Endo (n = 16), respectively, P < 0.05]. Our data suggest that reduced I(Na) availability in ventricular Epi may contribute to its greater sensitivity to electrical depression and thus may contribute to the R-ST segment changes observed under a variety of clinical conditions including acute myocardial ischemia, severe hyperkalemia, and Brugada syndrome.
Figures




References
-
- Antzelevitch C The Brugada syndrome: ionic basis and arrhythmia mechanisms. J Cardiovasc Electrophysiol 12: 268–272, 2001. - PubMed
-
- Antzelevitch C, Brugada P, Borggrefe M, Brugada J, Brugada R, Corrado D, Gussak I, LeMarec H, Nademanee K, Perez Riera AR, Shimizu W, Schulze-Bahr E, Tan H, Wilde A. Brugada syndrome: report of the second consensus conference. Heart Rhythm 2: 429–440, 2005. - PubMed
-
- Billman GE Ro 40–5967, a novel calcium channel antagonist, protects against ventricular fibrillation. Eur J Pharmacol 229: 179–187, 1992. - PubMed
-
- Chen Q, Kirsch GE, Zhang D, Brugada R, Brugada J, Brugada P, Potenza D, Moya A, Borggrefe M, Breithardt G, Ortiz-Lopez R, Wang Z, Antzelevitch C, O'Brien RE, Schultze-Bahr E, Keating MT, Towbin JA, Wang Q. Genetic basis and molecular mechanisms for idiopathic ventricular fibrillation. Nature 392: 293–296, 1998. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous