

Cerebral perfusion in sepsis-associated delirium
- PMID: 18457586
- PMCID: PMC2481444
- DOI: 10.1186/cc6891
Cerebral perfusion in sepsis-associated delirium
Abstract
Introduction: The pathophysiology of sepsis-associated delirium is not completely understood and the data on cerebral perfusion in sepsis are conflicting. We tested the hypothesis that cerebral perfusion and selected serum markers of inflammation and delirium differ in septic patients with and without sepsis-associated delirium.
Methods: We investigated 23 adult patients with sepsis, severe sepsis, or septic shock with an extracranial focus of infection and no history of intracranial pathology. Patients were investigated after stabilisation within 48 hours after admission to the intensive care unit. Sepsis-associated delirium was diagnosed using the confusion assessment method for the intensive care unit. Mean arterial pressure (MAP), blood flow velocity (FV) in the middle cerebral artery using transcranial Doppler, and cerebral tissue oxygenation using near-infrared spectroscopy were monitored for 1 hour. An index of cerebrovascular autoregulation was calculated from MAP and FV data. C-reactive protein (CRP), interleukin-6 (IL-6), S-100beta, and cortisol were measured during each data acquisition.
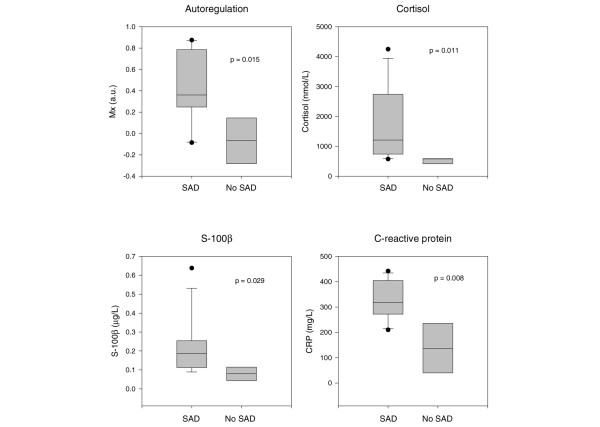
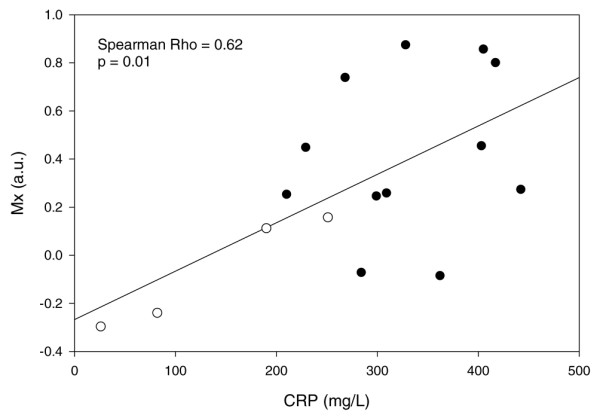
Results: Data from 16 patients, of whom 12 had sepsis-associated delirium, were analysed. There were no significant correlations or associations between MAP, cerebral blood FV, or tissue oxygenation and sepsis-associated delirium. However, we found a significant association between sepsis-associated delirium and disturbed autoregulation (P = 0.015). IL-6 did not differ between patients with and without sepsis-associated delirium, but we found a significant association between elevated CRP (P = 0.008), S-100beta (P = 0.029), and cortisol (P = 0.011) and sepsis-associated delirium. Elevated CRP was significantly correlated with disturbed autoregulation (Spearman rho = 0.62, P = 0.010).
Conclusion: In this small group of patients, cerebral perfusion assessed with transcranial Doppler and near-infrared spectroscopy did not differ between patients with and without sepsis-associated delirium. However, the state of autoregulation differed between the two groups. This may be due to inflammation impeding cerebrovascular endothelial function. Further investigations defining the role of S-100beta and cortisol in the diagnosis of sepsis-associated delirium are warranted.
Trial registration: ClinicalTrials.gov NCT00410111.
Figures
References
-
- Bleck TP, Smith MC, Pierre-Louis SJ, Jares JJ, Murray J, Hansen CA. Neurologic complications of critical medical illnesses. Crit Care Med. 1993;21:98–103. - PubMed
-
- Sprung CL, Peduzzi PN, Shatney CH, Schein RM, Wilson MF, Sheagren JN, Hinshaw LB. Impact of encephalopathy on mortality in the sepsis syndrome. The Veterans Administration Systemic Sepsis Cooperative Study Group. Crit Care Med. 1990;18:801–806. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
