

Radiofrequency ablation versus nephron-sparing surgery for small unilateral renal cell carcinoma: cost-effectiveness analysis
- PMID: 18458248
- PMCID: PMC5410944
- DOI: 10.1148/radiol.2481071448
Radiofrequency ablation versus nephron-sparing surgery for small unilateral renal cell carcinoma: cost-effectiveness analysis
Abstract
Purpose: To evaluate the relative cost-effectiveness of percutaneous radiofrequency (RF) ablation versus nephron-sparing surgery (NSS) in patients with small (<or=4-cm) renal cell carcinoma (RCC), given a commonly accepted level of societal willingness to pay.
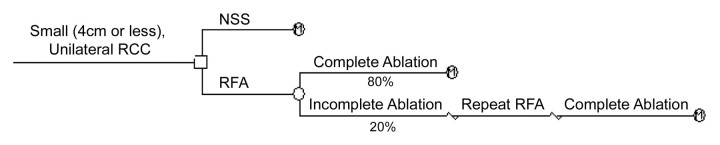
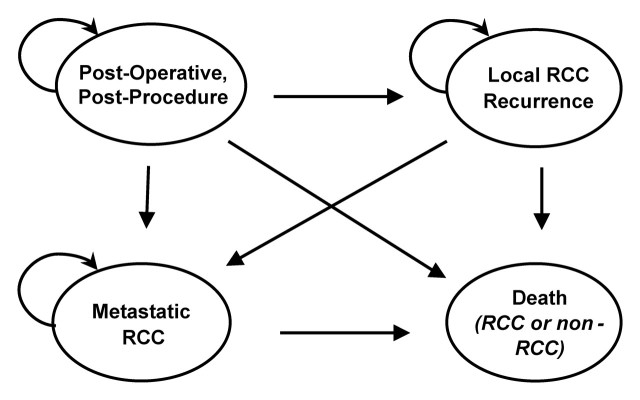
Materials and methods: A decision-analytic Markov model was developed to estimate life expectancy and lifetime costs for 65-year-old patients with a small RCC treated with RF ablation or NSS. The model incorporated RCC presence, treatment effectiveness and costs, and short- and long-term outcomes. An incremental cost-effectiveness analysis was performed to identify treatment preference under an assumed $75,000 per quality-adjusted life-year (QALY) societal willingness-to-pay threshold level, within proposed ranges for guiding implementation of new health care interventions. The effect of changes in key parameters on strategy preference was addressed in sensitivity analysis.
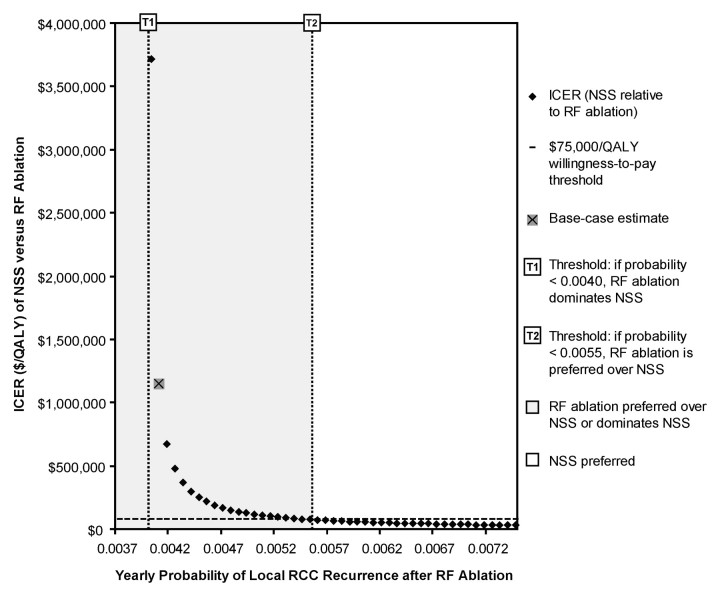
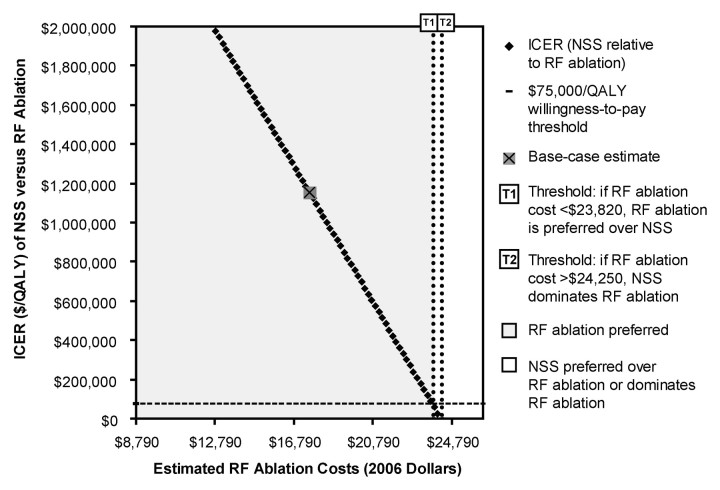
Results: By using base-case assumptions, NSS yielded a minimally greater average quality-adjusted life expectancy than did RF ablation (2.5 days) but was more expensive. NSS had an incremental cost-effectiveness ratio of $1,152,529 per QALY relative to RF ablation, greatly exceeding $75,000 per QALY. Therefore, RF ablation was considered preferred and remained so if the annual probability of post-RF ablation local recurrence was up to 48% higher relative to that post-NSS. NSS preference required an estimated NSS cost reduction of $7500 or RF ablation cost increase of $6229. Results were robust to changes in most model parameters, but treatment preference was dependent on the relative probabilities of local recurrence after RF ablation and NSS, the short-term costs of both, and quality of life after NSS.
Conclusion: RF ablation was preferred over NSS for small RCC treatment at a societal willingness-to-pay threshold level of $75,000 per QALY. This result was robust to changes in most model parameters, but somewhat dependent on the relative probabilities of post-RF ablation and post-NSS local recurrence, NSS and RF ablation short-term costs, and post-NSS quality of life, factors which merit further primary investigation.
(c) RSNA, 2008.
Figures

Comment in
-
Is radiofrequency ablation more cost-effective than nephron-sparing surgery for small unilateral renal cell carcinoma?Nat Clin Pract Urol. 2009 Jan;6(1):6-7. doi: 10.1038/ncpuro1239. Epub 2008 Oct 28. Nat Clin Pract Urol. 2009. PMID: 18957944
Similar articles
-
Active Surveillance Versus Nephron-Sparing Surgery for a Bosniak IIF or III Renal Cyst: A Cost-Effectiveness Analysis.AJR Am J Roentgenol. 2019 Apr;212(4):830-838. doi: 10.2214/AJR.18.20415. Epub 2019 Feb 19. AJR Am J Roentgenol. 2019. PMID: 30779659
-
Renal mass biopsy to guide treatment decisions for small incidental renal tumors: a cost-effectiveness analysis.Radiology. 2010 Sep;256(3):836-46. doi: 10.1148/radiol.10092013. Radiology. 2010. PMID: 20720070 Free PMC article.
-
Metastatic colorectal carcinoma: cost-effectiveness of percutaneous radiofrequency ablation versus that of hepatic resection.Radiology. 2004 Dec;233(3):729-39. doi: 10.1148/radiol.2333032052. Radiology. 2004. PMID: 15564408
-
Open surgery for localized RCC.ScientificWorldJournal. 2007 Jan 22;7:742-52. doi: 10.1100/tsw.2007.142. ScientificWorldJournal. 2007. PMID: 17619756 Free PMC article. Review.
-
A critical analysis of the actual role of minimally invasive surgery and active surveillance for kidney cancer.Eur Urol. 2010 Feb;57(2):223-32. doi: 10.1016/j.eururo.2009.10.023. Epub 2009 Oct 20. Eur Urol. 2010. PMID: 19853989 Review.
Cited by
-
Is radiofrequency ablation more cost-effective than nephron-sparing surgery for small unilateral renal cell carcinoma?Nat Clin Pract Urol. 2009 Jan;6(1):6-7. doi: 10.1038/ncpuro1239. Epub 2008 Oct 28. Nat Clin Pract Urol. 2009. PMID: 18957944
-
Microwave tissue ablation: biophysics, technology, and applications.Crit Rev Biomed Eng. 2010;38(1):65-78. doi: 10.1615/critrevbiomedeng.v38.i1.60. Crit Rev Biomed Eng. 2010. PMID: 21175404 Free PMC article. Review.
-
Decision Making: Thermal Ablation Options for Small Renal Masses.Semin Intervent Radiol. 2017 Jun;34(2):167-175. doi: 10.1055/s-0037-1602708. Epub 2017 Jun 1. Semin Intervent Radiol. 2017. PMID: 28579684 Free PMC article. Review.
-
Percutaneous Image-guided Thermal Ablation for Renal Cell Carcinoma.Interv Radiol (Higashimatsuyama). 2020 Jun 30;5(2):32-42. doi: 10.22575/interventionalradiology.2020-0001. eCollection 2020 Jun 30. Interv Radiol (Higashimatsuyama). 2020. PMID: 36284654 Free PMC article. Review.
-
Radiofrequency ablation of renal tumours: diagnostic accuracy of contrast-enhanced ultrasound for early detection of residual tumour.Eur Radiol. 2010 Aug;20(8):1812-21. doi: 10.1007/s00330-010-1742-6. Epub 2010 Mar 4. Eur Radiol. 2010. PMID: 20204642
References
-
- American Cancer Society. Cancer facts and 2007 figures 2007. Atlanta, Ga: American Cancer Society, 2007.
-
- Chow WH, Devesa SS, Warren JL, Fraumeni JF Jr. Rising incidence of renal cell cancer in the United States. JAMA 1999;281:1628–1631. - PubMed
-
- Devesa SS, Silverman DT, McLaughlin JK, Brown CC, Connelly RR, Fraumeni JF Jr. Comparison of the descriptive epidemiology of urinary tract cancers. Cancer Causes Control 1990;1:133–141. - PubMed
-
- Jayson M, Sanders H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology 1998;51:203–205. - PubMed
-
- Hollingsworth JM, Miller DC, Daignault S, Hollenbeck BK. Rising incidence of small renal masses: a need to reassess treatment effect. J Natl Cancer Inst 2006;98:1331–1334. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
