

Selective serotonin reuptake inhibitors for unipolar depression: a systematic review of classic long-term randomized controlled trials
- PMID: 18458261
- PMCID: PMC2335186
- DOI: 10.1503/cmaj.071068
Selective serotonin reuptake inhibitors for unipolar depression: a systematic review of classic long-term randomized controlled trials
Abstract
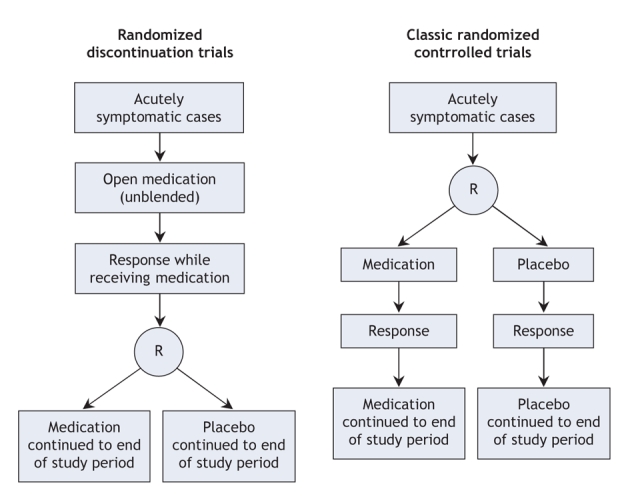
Background: Selective serotonin reuptake inhibitors are increasingly used in the long-term treatment of depression. Much of the supporting evidence about the effects of these drugs comes from discontinuation trials, a variant of randomized controlled trials whose design is problematic to interpret. We conducted a systematic review to examine the efficacy and acceptability of long-term therapy with selective serotonin reuptake inhibitors relative to placebo in the treatment of unipolar depression.
Methods: We identified placebo-controlled randomized trials with a treatment duration of at least 6 months by searching MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials to update a recently published systematic review. Efficacy was defined in terms of response to treatment (50% improvement in depression score relative to baseline) and remission (score of 7 or below on the Hamilton rating scale for depression). Key secondary outcomes included quality of life, return to work, need for additional treatment and self-harm. Overall acceptability was defined in terms of dropouts for any reason over a course of treatment.
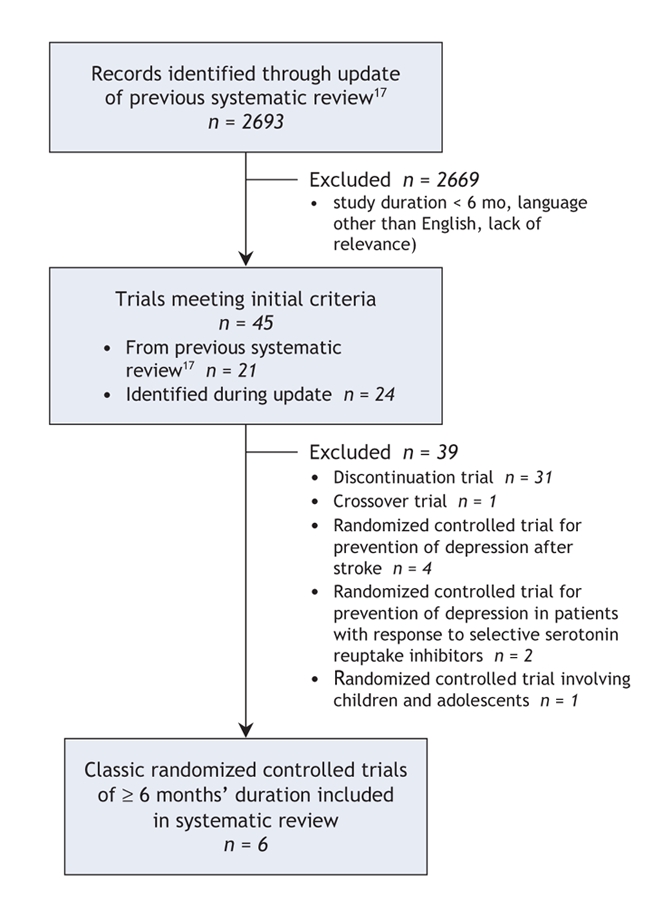
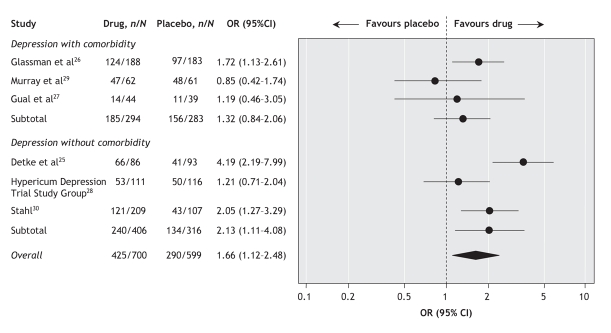
Results: Of the 2693 records identified initially, we included 6 randomized controlled trials that met our eligibility criteria. These studies had a moderate risk of bias, had assigned a total of 1299 participants with depression to either treatment or placebo and had followed both groups for 6-8 months. We observed statistically significant improvements in response to treatment (odds ratio [OR] 1.66, 95% confidence interval [CI] 1.12-2.48), but not in remission (OR 1.46, 95% CI 0.92-2.32) or acceptability (OR 0.87, 95% CI 0.67-1.14). The effects appeared greater among patients without comorbidities.
Interpretation: There is a lack of classic randomized controlled trials of serotonin reuptake inhibitors lasting more than 1 year for the treatment of depression. The results of our systematic review support current recommendations for 6-8 months of antidepressant treatment following initial recovery but provide no guidance for longer treatment.
Figures


Comment in
-
Bringing a research base to psychiatry.CMAJ. 2008 May 6;178(10):1257-60. doi: 10.1503/cmaj.080530. CMAJ. 2008. PMID: 18458250 Free PMC article. No abstract available.
-
Developing the evidence for evidence-based practice.CMAJ. 2008 May 6;178(10):1313-5. doi: 10.1503/cmaj.080202. CMAJ. 2008. PMID: 18458263 Free PMC article. No abstract available.
References
-
- Raymond CB, Morgan SG, Caetano PA. Antidepressant utilization in British Columbia from 1996 to 2004: increasing prevalence but not incidence. Psychiatr Serv 2007;58:79-84. - PubMed
-
- Petty DR, House A, Knapp P, et al. Prevalence, duration and indications for prescribing of antidepressants in primary care. Age Ageing 2006;35:523-6. - PubMed
-
- Meijer WE, Heerdink ER, Leufkens HG, et al. Incidence and determinants of long-term use of antidepressants. Eur J Clin Pharmacol 2004;60:57-61. - PubMed
-
- Depression: management of depression in primary and secondary care. London (UK): National Institute for Health and Clinical Excellence; 2004.
-
- Major depression in adults in primary care. Bloomington (MN): Institute for Clinical Systems Improvement; 2006.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous