

Trends in mortality, complications, and demographics for primary hip arthroplasty in the United States
- PMID: 18461326
- PMCID: PMC2903109
- DOI: 10.1007/s00264-008-0549-4
Trends in mortality, complications, and demographics for primary hip arthroplasty in the United States
Abstract
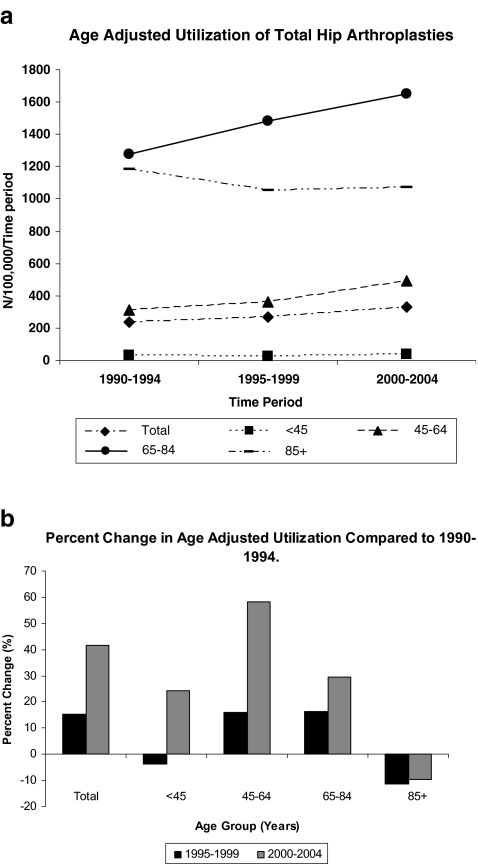
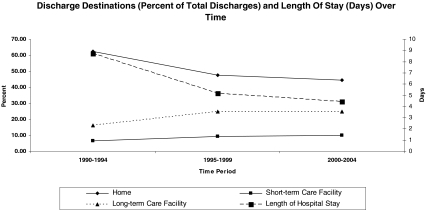
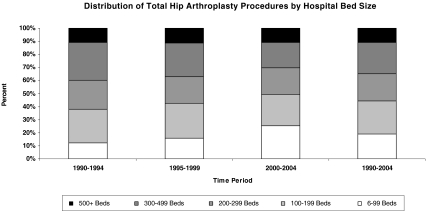
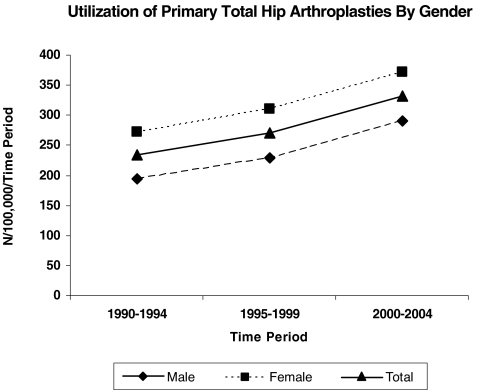
To determine trends in characteristics of total hip arthroplasty (THA) in the United States, the National Hospital Discharge Survey (NHDS) was analyzed from 1990 to 2004 for trends in in-hospital mortality and complications, length of hospital stay, demographics, and comorbidities. The number of THAs performed increased by 158%, whereas mortality rates remained low and slightly decreased (from 0.32% to 0.29%). Prevalence of procedure-related complications decreased over time, and length of stay decreased from an average of 8.7 days to 4.5 days. These improvements occurred despite an increase in comorbidities in patients. An increase in both the proportion of discharges to long- and short-term care facilities and in the proportion of procedures performed in smaller hospitals was noted. Multiple temporal changes in outcomes and demographics for THA were found. These changes have implications for clinical care and allocation of health resources.
Le but de ce travail est de mettre en évidence les nouvelles données caractéristiques des prothèses totales de hanche aux Etats-Unis. Matériel et méthode: Le National Hospital Discharge Survey (NHDS) a été analysé durant la période de 1990 à 2004 sur le plan de la mortalité, des complications, de la durée de séjour, sur le plan démographique et des comorbidités. Résultat: le nombre de prothèses totales de hanche a augmenté de 158% dans cette période alors que la mortalité reste basse et a même légèrement diminué (0,32% à 0,29%). Le taux de complications et la durée moyenne de séjour diminuent également avec le temps de 8,7 jours à 4,5 jours. Ces améliorations entraînent néanmoins une augmentation des comorbidités chez les patients. Il a été noté une augmentation de la proportion des sorties avec prise en charge des soins de courte ou longue durée et une proportion importante de procédures réalisées dans les petits hôpitaux. les modifications notées sur le devenir et sur les bases démographiques des prothèses totales de hanche, ont une implication clinique sur les soins et sur l’allocation de ressource.
Figures
Comment in
-
Rehabilitation therapy reduces mortality after total hip replacements.Int Orthop. 2014 Apr;38(4):911. doi: 10.1007/s00264-013-2198-5. Epub 2013 Nov 24. Int Orthop. 2014. PMID: 24271335 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention (2007) Selected articles using National Hospital Discharge Survey (NHDS) or National Survey of Ambulatory Surgery (NSAS) data. http://www.cdc.gov/nchs/data/hdasd/NHDS2007articleupdate.pdf. Accessed 10 March 2008
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
