

Influence of CYP2C9 and VKORC1 on warfarin dose, anticoagulation attainment and maintenance among European-Americans and African-Americans
- PMID: 18466099
- PMCID: PMC2757655
- DOI: 10.2217/14622416.9.5.511
Influence of CYP2C9 and VKORC1 on warfarin dose, anticoagulation attainment and maintenance among European-Americans and African-Americans
Abstract
Aims: The influence of CYP2C9 and VKORC1 on warfarin dose, time to target International Normalized Ratio (INR), time to stabilization, and risk of over-anticoagulation (INR: > 4) was assessed after adjustment for clinical factors, intraindividual variation in environmental factors and unobserved heterogeneity.
Materials & methods: Common CYP2C9 and VKORC1 polymorphisms were assessed in 302 European-Americans and 273 African-Americans receiving warfarin. Race-stratified multivariable analyses evaluated the influence of CYP2C9 and VKORC1 on warfarin response.
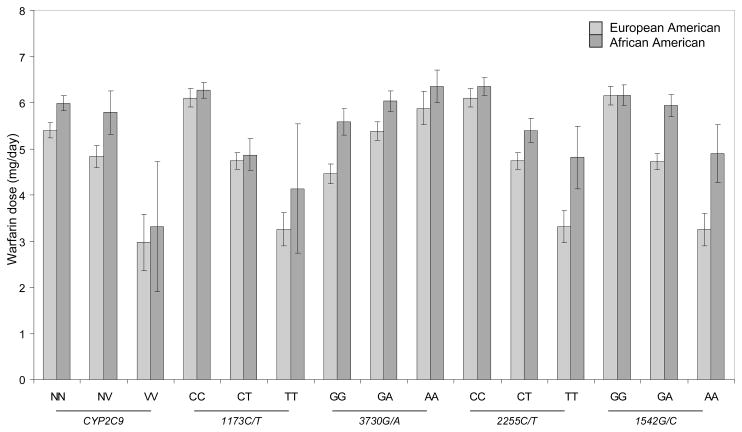
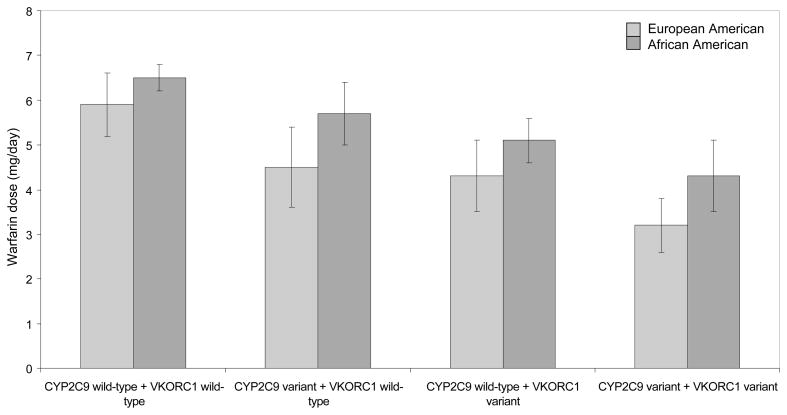
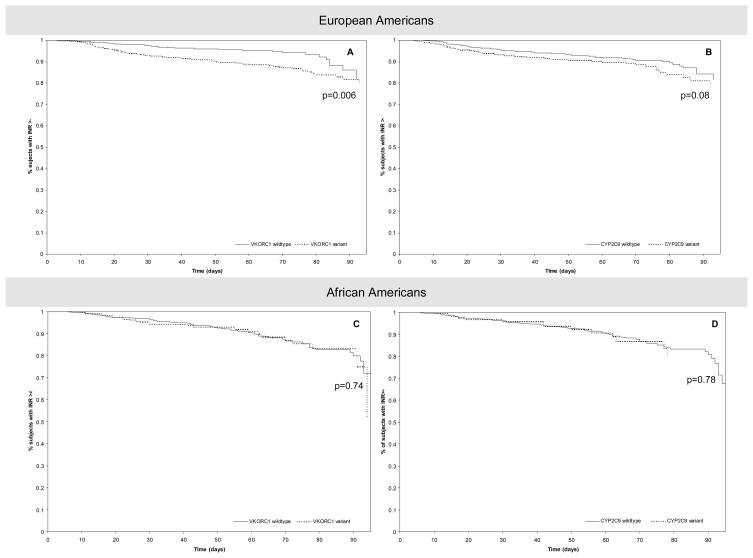
Results & conclusion: CYP2C9 and VKORC1 accounted for up to 30% of the variability in warfarin dose among European-Americans and 10% among African-Americans. Neither CYP2C9 nor VKORC1 influenced the time to target INR or stabilization among patients of either race, and neither influenced the risk of over-anticoagulation among African-Americans. The risk of over-anticoagulation was higher among European-Americans with variant VKORC1 1173C/T (p < 0.01) and marginally significant among those with variant CYP2C9 (p = 0.08) genotype. Although CYP2C9 and VKORC1 genotyping can facilitate individualized initiation of warfarin dose in African and European-Americans, the ability to predict the risk of over-anticoagulation is inconsistent across race. Identification of other factors that can predict such risk consistently in a racially diverse group will facilitate individualized maintenance of warfarin therapy.
Figures
References
-
- Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154:1449–57. - PubMed
-
- Hirsh J, Dalen J, Anderson DR, et al. Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest. 2001;119:8S–21S. - PubMed
-
- Hylek EM, D’Antonio J, Evans-Molina C, Shea C, Henault LE, Regan S. Translating the results of randomized trials into clinical practice: the challenge of warfarin candidacy among hospitalized elderly patients with atrial fibrillation. Stroke. 2006;37:1075–80. - PubMed
-
- Stafford RS, Radley DC. The underutilization of cardiac medications of proven benefit, 1990 to 2002. J Am Coll Cardiol. 2003;41:56–61. - PubMed
-
- Tapson VF, Hyers TM, Waldo AL, et al. Antithrombotic therapy practices in US hospitals in an era of practice guidelines. Arch Intern Med. 2005;165:1458–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials