

Breast cancer tumor growth estimated through mammography screening data
- PMID: 18466608
- PMCID: PMC2481488
- DOI: 10.1186/bcr2092
Breast cancer tumor growth estimated through mammography screening data
Abstract
Introduction: Knowledge of tumor growth is important in the planning and evaluation of screening programs, clinical trials, and epidemiological studies. Studies of tumor growth rates in humans are usually based on small and selected samples. In the present study based on the Norwegian Breast Cancer Screening Program, tumor growth was estimated from a large population using a new estimating procedure/model.
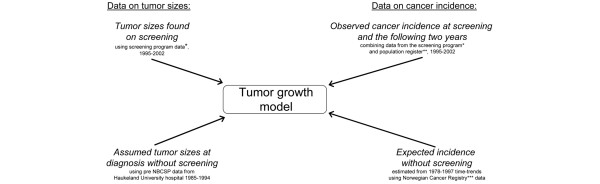
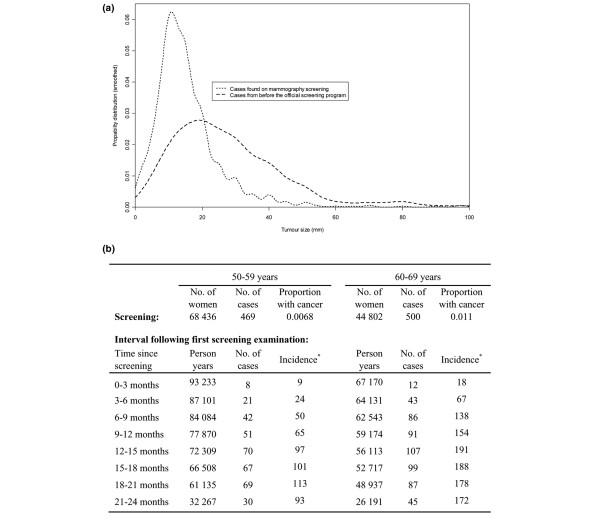
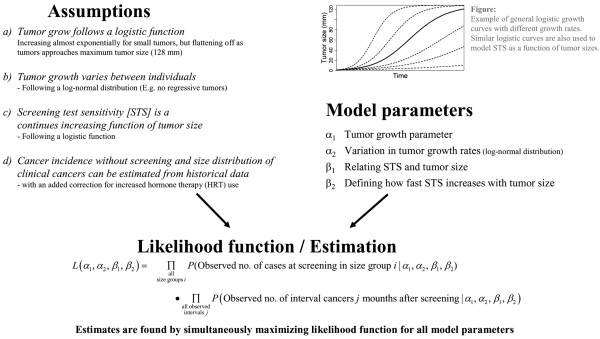
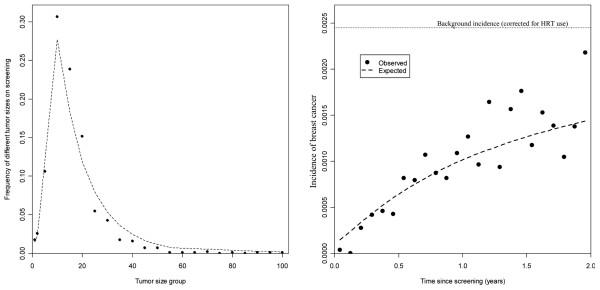
Methods: A likelihood-based estimating procedure was used, where both tumor growth and the screen test sensitivity were modeled as continuously increasing functions of tumor size. The method was applied to cancer incidence and tumor measurement data from 395,188 women aged 50 to 69 years.
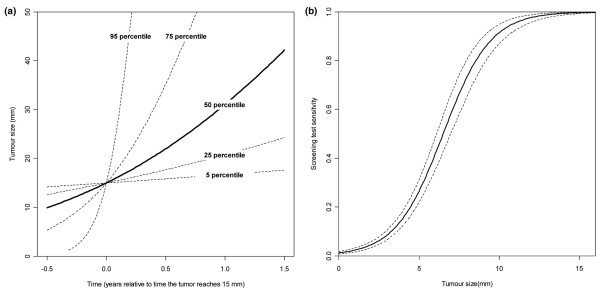
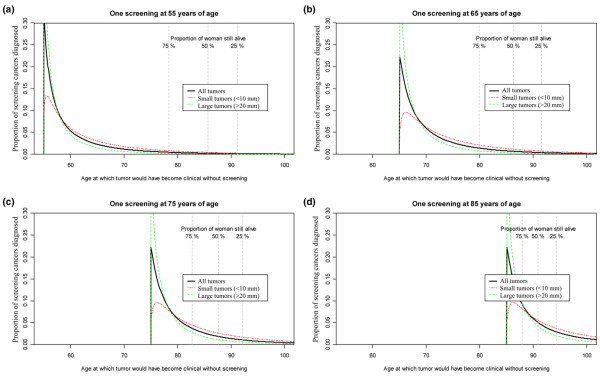
Results: Tumor growth varied considerably between subjects, with 5% of tumors taking less than 1.2 months to grow from 10 mm to 20 mm in diameter, and another 5% taking more than 6.3 years. The mean time a tumor needed to grow from 10 mm to 20 mm in diameter was estimated as 1.7 years, increasing with age. The screen test sensitivity was estimated to increase sharply with tumor size, rising from 26% at 5 mm to 91% at 10 mm. Compared with previously used Markov models for tumor progression, the applied model gave considerably higher model fit (85% increased predictive power) and provided estimates directly linked to tumor size.
Conclusion: Screening data with tumor measurements can provide population-based estimates of tumor growth and screen test sensitivity directly linked to tumor size. There is a large variation in breast cancer tumor growth, with faster growth among younger women.
Figures
References
-
- Prevost TC, Launoy G, Duffy SW, Chen HH. Estimating sensitivity and sojourn time in screening for colorectal cancer: a comparison of statistical approaches. Am J Epidemiol. 1998;148:609–619. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
