

An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial
- PMID: 18468543
- PMCID: PMC2387195
- DOI: 10.1016/S0140-6736(08)60692-3
An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial
Abstract
Background: Schools in many countries undertake programmes for smoking prevention, but systematic reviews have shown mixed evidence of their effectiveness. Most peer-led approaches have been classroom-based, and rigorous assessments are scarce. We assessed the effectiveness of a peer-led intervention that aimed to prevent smoking uptake in secondary schools.
Methods: We undertook a cluster randomised controlled trial of 10 730 students aged 12-13 years in 59 schools in England and Wales. 29 schools (5372 students) were randomly assigned by stratified block randomisation to the control group to continue their usual smoking education and 30 (5358 students) to the intervention group. The intervention (ASSIST [A Stop Smoking In Schools Trial] programme) consisted of training influential students to act as peer supporters during informal interactions outside the classroom to encourage their peers not to smoke. Follow-up was immediately after the intervention and at 1 and 2 years. Primary outcomes were smoking in the past week in both the school year group and in a group at high risk of regular smoking uptake, which was identified at baseline as occasional, experimental, or ex-smokers. Analysis was by intention to treat. This study is registered, number ISRCTN55572965.
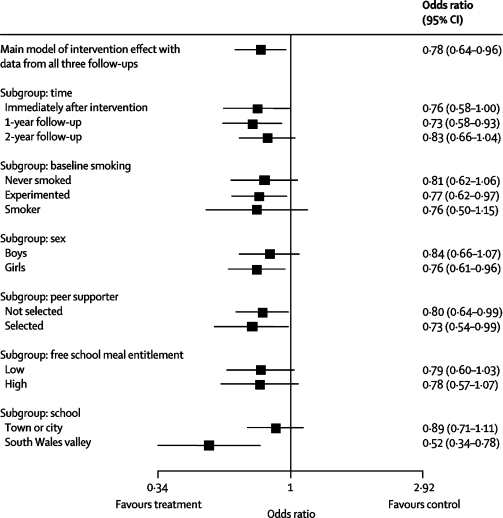
Findings: The odds ratio of being a smoker in intervention compared with control schools was 0.75 (95% CI 0.55-1.01) immediately after the intervention (n=9349 students), 0.77 (0.59-0.99) at 1-year follow-up (n=9147), and 0.85 (0.72-1.01) at 2-year follow-up (n=8756). The corresponding odds ratios for the high-risk group were 0.79 (0.55-1.13 [n=3561]), 0.75 (0.56-0.99 [n=3483]), and 0.85 (0.70-1.02 [n=3294]), respectively. In a three-tier multilevel model with data from all three follow-ups, the odds of being a smoker in intervention compared with control schools was 0.78 (0.64-0.96).
Interpretation: The results suggest that, if implemented on a population basis, the ASSIST intervention could lead to a reduction in adolescent smoking prevalence of public-health importance.
Figures

Comment in
-
Moving tobacco prevention outside the classroom.Lancet. 2008 May 10;371(9624):1556-7. doi: 10.1016/S0140-6736(08)60668-6. Lancet. 2008. PMID: 18468528 Clinical Trial. No abstract available.
References
-
- Warren CW, Jones NR, Eriksen MP, Asma S, for the Global Tobacco Surveillance System (GTSS) collaborative group Patterns of global tobacco use in young people and implications for future chronic disease burden in adults. Lancet. 2006;367:749–753. - PubMed
-
- Peto R, Lopez AD. The future worldwide health effects of current smoking patterns. In: Boyle P, Gray N, Henningfield J, Seffrin J, Zatonski W, editors. Tobacco and public health: science and policy. Oxford University Press; Oxford: 2004. pp. 281–286.
-
- DiFranza JR, Savageau JA, Fletcher K. Symptoms of tobacco dependence after brief intermittent use. The development and assessment of nicotine dependence in youth–2 study. Arch Pediatr Adolesc Med. 2007;161:704–710. - PubMed
-
- Taioli E, Wynder EL. Effect of the age at which smoking begins on frequency of smoking in adulthood. N Engl J Med. 1991;325:968–969. - PubMed
-
- Chassin L, Presson CC, Pitts SC, Sherman SJ. The natural history of cigarette smoking from adolescence to adulthood in a Midwestern community sample: multiple trajectories and their psychosocial correlates. Health Psychology. 2000;19:223–231. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
