

Survival rates after resection for localized kidney cancer: 1989 to 2004
- PMID: 18470927
- PMCID: PMC3985136
- DOI: 10.1002/cncr.23520
Survival rates after resection for localized kidney cancer: 1989 to 2004
Abstract
Background: Mortality rates from kidney cancer have continued to rise despite increases in the detection of smaller renal tumors and rates of renal surgery. To explore the factors associated with this treatment-outcome discrepancy, the authors evaluated how changes in tumor size have affected disease progression in patients after nephrectomy for localized kidney cancer, and they sought to identify the factors associated with disease progression and overall patient survival after resection for localized kidney cancer.
Methods: In total, 1618 patients with localized kidney cancer were identified who underwent nephrectomy at Memorial Sloan-Kettering Cancer Center from 1989 to 2004. Patients were categorized by year of surgery: from 1989 to 1992, from 1993 to 1996, from 1997 to 2000, and from 2001 to 2004. Tumor size was classified according to the following strata: <2 cm, from 2 cm to 4 cm, from 4 cm to 7 cm, and >7 cm. Disease progression was defined as the development of local recurrence or distant metastases. Five-year progression-free survival (PFS) was calculated for patients in each tumor size strata according to the year of operation using the Kaplan-Meier method. The patient-, tumor-, and surgery-related characteristics associated with PFS and overall survival (OS) were explored using univariate analysis, and all significant variables were retained in a multivariate Cox regression analysis.
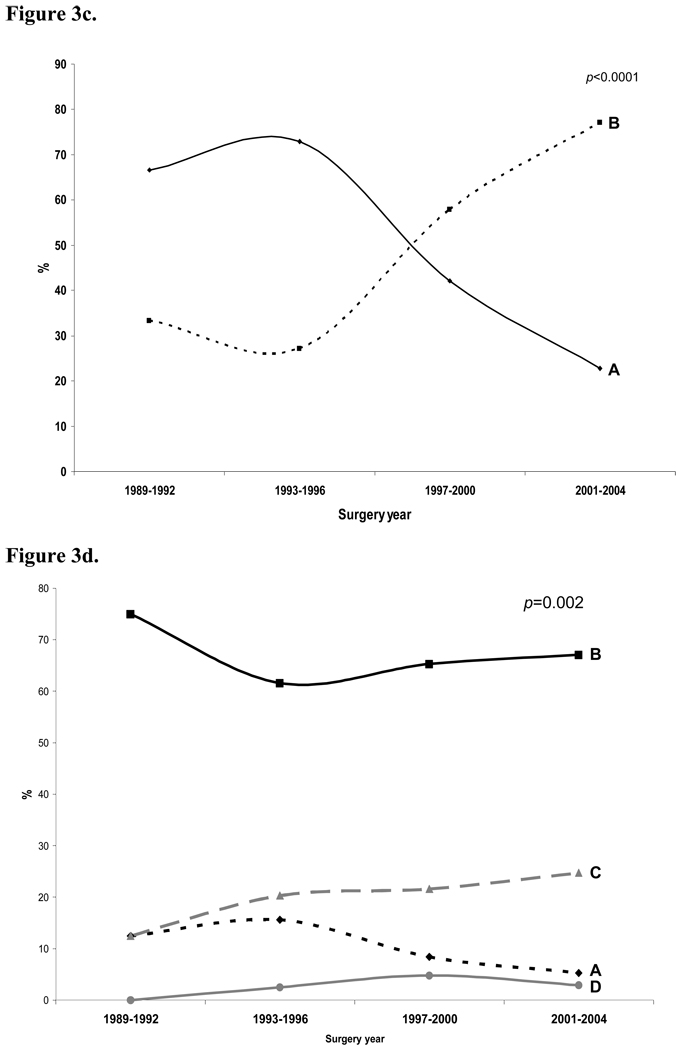
Results: Overall, the number of nephrectomies increased for all tumor size categories from 1989 to 2004. A tumor size migration was evident during this period, because the proportion of patients with tumors <2 cm and with tumors from 2 cm to 4 cm increased, whereas the proportion of patients with tumors >7 cm decreased. One hundred seventy-nine patients (11%) developed disease progression after nephrectomy. Sixteen patients (1%) developed local recurrences, and 163 patients (10%) developed distant metastases. When 5-year PFS was calculated for each tumor size strata according to 4-year cohorts, trends in PFS did not improve or differ significantly over time. Compared with historic cohorts, patients in more contemporary cohorts were more likely to undergo partial nephrectomy rather than radical nephrectomy and were less likely to undergo concomitant lymph node dissection and adrenalectomy. Multivariate analysis demonstrated that pathologic stage and tumor grade were associated with disease progression, whereas patient age and tumor stage were associated with overall patient survival.
Conclusions: Despite an increasing number of nephrectomies and a size migration toward smaller tumors, trends in 5-year PFS and OS did not improve or differ significantly over time. These findings require further research to identify causative mechanisms, and they argue for the consideration of active surveillance for patients who have select renal tumors and a re-evaluation of the current treatment paradigm of surgically removing solid renal masses on initial detection.
(Copyright) 2008 American Cancer Society.
Conflict of interest statement
We declare no conflicts of interest.
Figures








References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57(1):43–66. - PubMed
-
- Chow WH, Devesa SS, Warren JL, Fraumeni JF., Jr Rising incidence of renal cell cancer in the United States. Jama. 1999;281(17):1628–1631. - PubMed
-
- Volpe A, Panzarella T, Rendon RA, Haider MA, Kondylis FI, Jewett MA. The natural history of incidentally detected small renal masses. Cancer. 2004;100(4):738–745. - PubMed
-
- Lee CT, Katz J, Shi W, Thaler HT, Reuter VE, Russo P. Surgical management of renal tumors 4 cm. or less in a contemporary cohort. J Urol. 2000;163(3):730–736. - PubMed
-
- Tsui KH, Shvarts O, Smith RB, Figlin R, de Kernion JB, Belldegrun A. Renal cell carcinoma: prognostic significance of incidentally detected tumors. J Urol. 2000;163(2):426–430. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
