

A randomized, prospective, double-blind, placebo-controlled trial of terlipressin for type 1 hepatorenal syndrome
- PMID: 18471513
- PMCID: PMC3730280
- DOI: 10.1053/j.gastro.2008.02.014
A randomized, prospective, double-blind, placebo-controlled trial of terlipressin for type 1 hepatorenal syndrome
Abstract
Background & aims: Hepatorenal syndrome (HRS) type 1 is a progressive functional renal failure in subjects with advanced liver disease. The aim of this study was to evaluate the efficacy and safety of terlipressin, a systemic arterial vasoconstrictor, for cirrhosis type 1 HRS.
Methods: A prospective, randomized, double-blind, placebo-controlled clinical trial of terlipressin was performed. Subjects with type 1 HRS were randomized to terlipressin (1 mg intravenously every 6 hours) or placebo plus albumin in both groups. The dose was doubled on day 4 if the serum creatinine (SCr) level did not decrease by 30% of baseline. Treatment was continued to day 14 unless treatment success, death, dialysis, or transplantation occurred. Treatment success was defined by a decrease in SCr level to </=1.5 mg/dL for at least 48 hours by day 14 without dialysis, death, or relapse of HRS type 1.
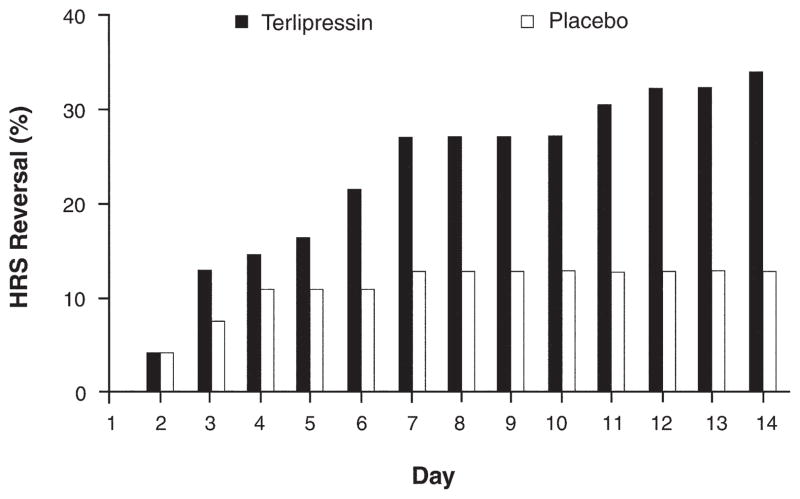
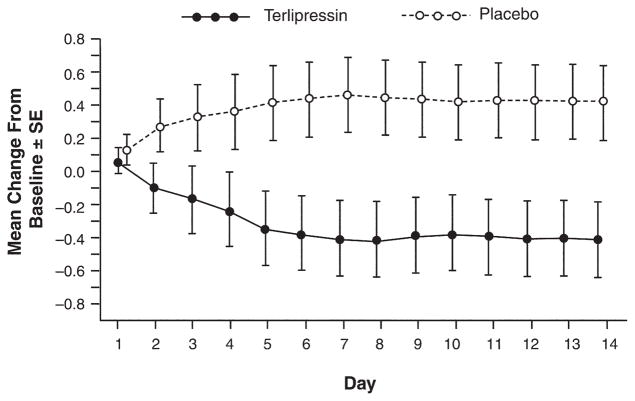
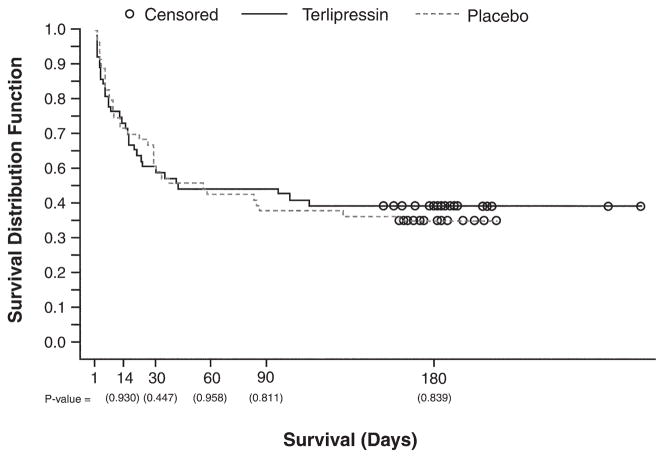
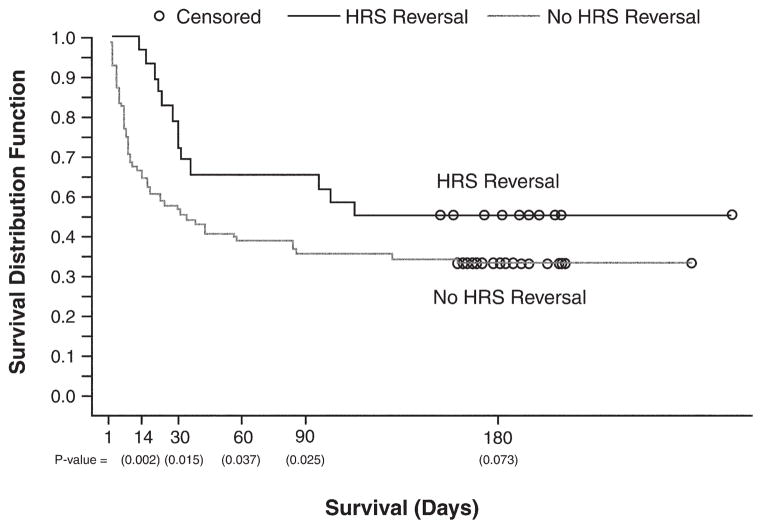
Results: Fifty-six subjects were randomized to each arm. Treatment success with terlipressin was double that with placebo (25% vs 12.5%, P = .093). SCr level improved from baseline to day 14 on terlipressin (-0.7 mg/dL) as compared with placebo (0 mg/dL), P < .009. Terlipressin was superior to placebo for HRS reversal (34% vs 13%, P = .008), defined by decrease in SCr level </=1.5 mg/dL. Overall and transplantation-free survival was similar between study groups; HRS reversal significantly improved survival at day 180. One nonfatal myocardial infarction occurred with terlipressin, but the total adverse event rate was similar to placebo.
Conclusions: Terlipressin is an effective treatment to improve renal function in HRS type 1.
Trial registration: ClinicalTrials.gov NCT00089570.
Conflict of interest statement
Conflicts of interest and financial disclosures: Arun J. Sanyal, MBBS, MD: Stipends paid by Orphan Therapeutics to maintain the 24-hour study Medical Hotline (June 2004, $12,000; May 2005, $12,000). Reimbursement for travel costs and data reviews for FDA meetings (2006, $501.90; April 2007, $251.67). Thomas Boyer, MD: Reimbursement for travel costs and data reviews for FDA meetings (February 2004, $1157.90; June 2006, $377.70; October 2006, $699.20; March 2007, $389.60). Honorarium for OT-0401 Steering Committee in 2004 ($1350.00). Guadalupe Garcia-Tsao, MD: Honorarium for OT-0401 Steering Committee in 2004 ($750.00). Frederick Regenstein, MD: Honorarium for OT-0401 Steering Committee in 2004 ($750.00). Lorenzo Rossaro, MD: Honorarium for OT-0401 Steering Committee in 2004 ($750.00). Andres Blei, MD: None. Veit Gülberg, MD: None. Beate Appenrodt, MD: None. Samuel Sigal, MD: None. Peter Teuber, PhD: President and Managing Partner of Orphan Therapeutics, LLC (OT-0401 study cosponsor).
Figures
Comment in
-
Vasoconstrictor therapy for the hepatorenal syndrome.Gastroenterology. 2008 May;134(5):1608-11. doi: 10.1053/j.gastro.2008.03.034. Gastroenterology. 2008. PMID: 18471529 No abstract available.
-
[Terlipressin for hepatorenal syndrome - what is the role of plasma expansion and hemodynamic monitoring?].Z Gastroenterol. 2009 Mar;47(3):307-8. doi: 10.1055/s-0028-1109113. Epub 2009 Mar 11. Z Gastroenterol. 2009. PMID: 19280545 German. No abstract available.
-
Terlipressin for hepatorenal syndrome: continuous infusion as an alternative to i.v. bolus administration.Gastroenterology. 2009 Sep;137(3):1179; author reply 1179-81. doi: 10.1053/j.gastro.2009.03.064. Epub 2009 Jul 23. Gastroenterology. 2009. PMID: 19631603 No abstract available.
References
-
- Alessandria C, Ozdogan O, Guevara M, et al. MELD score and clinical type predict prognosis in hepatorenal syndrome: relevance to liver transplantation. Hepatology. 2005;41:1282–1289. - PubMed
-
- Gines A, Escorsell A, Gines P, et al. Incidence, predictive factors, and prognosis of the hepatorenal syndrome in cirrhosis with ascites. Gastroenterology. 1993;105:229–236. - PubMed
-
- Arroyo V, Terra C, Gines P. Advances in the pathogenesis and treatment of type-1 and type-2 hepatorenal syndrome. J Hepatol. 2007;46:935–946. - PubMed
-
- Rimola A, Gines P, Arroyo V, et al. Urinary excretion of 6-keto-prostaglandin F1 α, thromboxane B2 and prostaglandin E2 in cirrhosis with ascites. Relationship to functional renal failure (hepatorenal syndrome) J Hepatol. 1986;3:111–117. - PubMed
-
- Moller S, Abrahamsen J, Ring-Larsen H, et al. The hepatorenal syndrome. Ugeskrift for laeger. 1995;157:3185–3189. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
