

Borderline resectable pancreatic cancer: the importance of this emerging stage of disease
- PMID: 18471707
- PMCID: PMC5901743
- DOI: 10.1016/j.jamcollsurg.2007.12.020
Borderline resectable pancreatic cancer: the importance of this emerging stage of disease
Abstract
Background: Patients with borderline resectable pancreatic adenocarcinoma (PA) include those with localized disease who have tumor or patient characteristics that preclude immediate surgery. There is no optimal treatment schema for this distinct stage of disease, so the role of surgery is undefined.
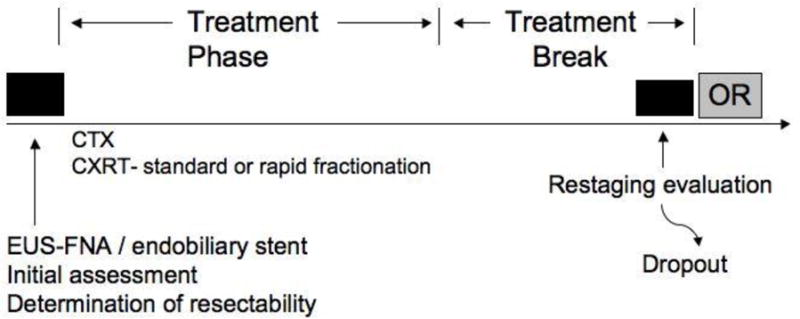
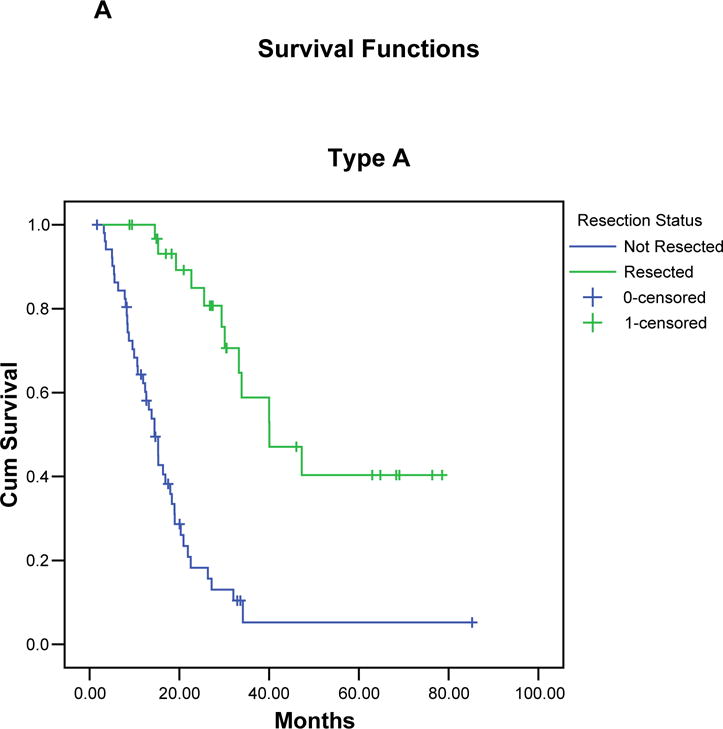
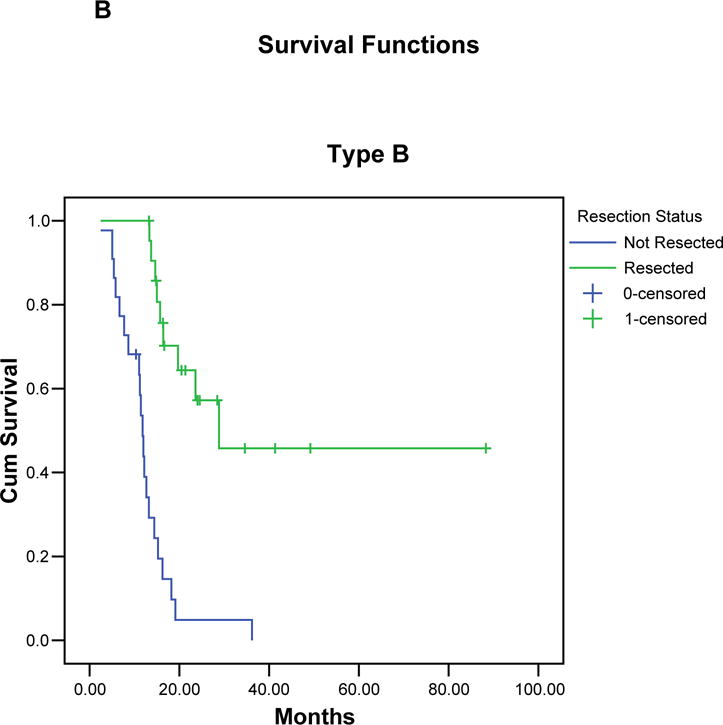
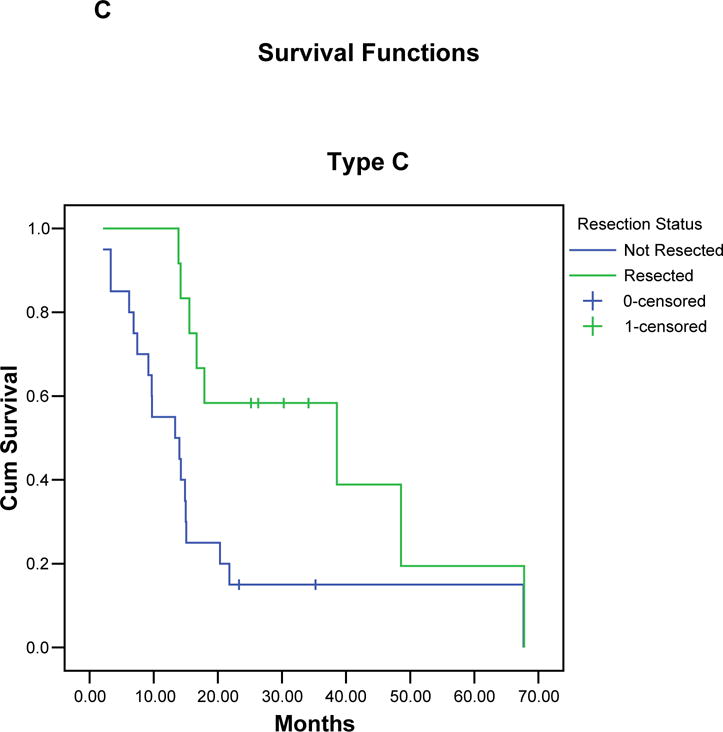
Study design: We defined patients with borderline resectable PA as fitting into one of three distinct groups. Group A comprised patients with tumor abutment of the visceral arteries or short-segment occlusion of the Superior Mesenteric Vein. In group B, patients had findings suggestive but not diagnostic of metastasis. Group C patients were of marginal performance status. Patients were treated initially with chemotherapy, chemoradiation, or both; those of sufficient performance status who completed preoperative therapy without disease progression were considered for surgery.
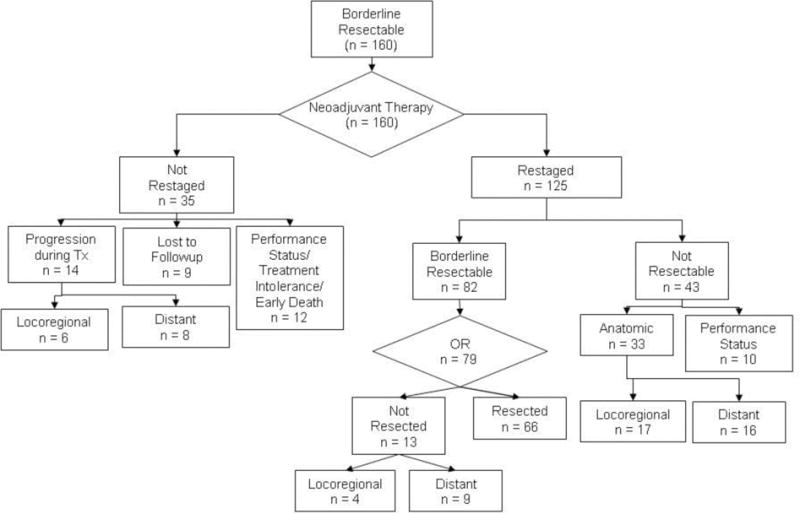
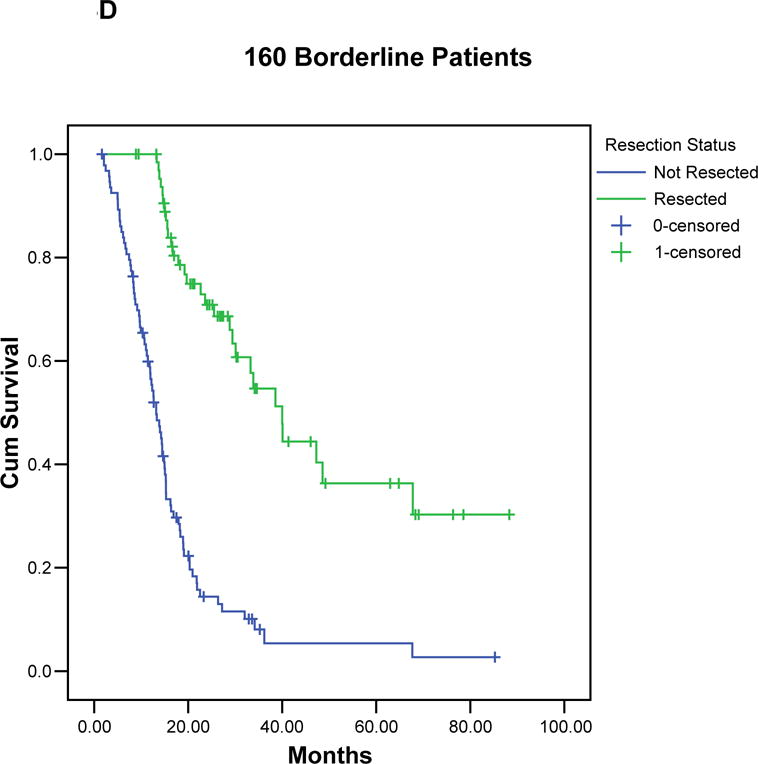
Results: Between October 1999 and August 2006, 160 (7%) of 2,454 patients with PA were classified as borderline resectable. Of these, 125 (78%) completed preoperative therapy and restaging, and 66 (41%) underwent pancreatectomy. Vascular resection was required in 18 (27%) of 66 patients, and 62 (94%) underwent a margin-negative pancreatectomy. A partial pathologic response to induction therapy (< 50% viable tumor) was seen in 37 (56%) of 66 patients. Median survival was 40 months for the 66 patients who completed all therapy and 13 months for the 94 patients who did not undergo pancreatectomy (p < 0.001).
Conclusions: This is the first large report of borderline resectable PA and includes objective definitions for this stage of disease. Our neoadjuvant approach allowed for identification of the marked subset of patients that was most likely to benefit from surgery, as evidenced by the favorable median survival in this group.
Figures
References
-
- Wolff RA, Crane C, Li D, Abbruzzese JL, Evans DB. Neoplasms of the exocrine pancreas. In: Kufe DW, et al., editors. Cancer Medicine. 8th. BC Decker; London: 2006. pp. 1331–1358.
-
- National Comprehensive Cancer Network (NCCN) practice guidelines for pancreatic cancer. 2004
-
- Varadhachary GR, et al. Borderline resectable pancreatic cancer: definitions, management, and role of preoperative therapy. Annals of surgical oncology. 2006;13:1035–1046. - PubMed
-
- Oken MM, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. American Journal of Clinical Oncology. 1982;5:649–655. - PubMed
