

Amyloidogenic and associated proteins in systemic amyloidosis proteome of adipose tissue
- PMID: 18474516
- PMCID: PMC2494907
- DOI: 10.1074/mcp.M700545-MCP200
Amyloidogenic and associated proteins in systemic amyloidosis proteome of adipose tissue
Abstract
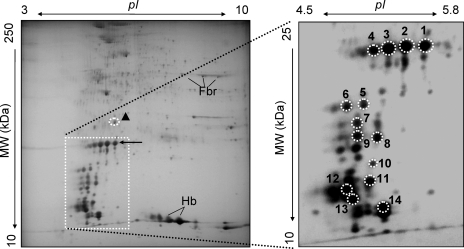
In systemic amyloidoses, widespread deposition of protein as amyloid causes severe organ dysfunction. It is necessary to discriminate among the different forms of amyloid to design an appropriate therapeutic strategy. We developed a proteomics methodology utilizing two-dimensional polyacrylamide gel electrophoresis followed by matrix-assisted laser desorption/ionization mass spectrometry and peptide mass fingerprinting to directly characterize amyloid deposits in abdominal subcutaneous fat obtained by fine needle aspiration from patients diagnosed as having amyloidoses typed as immunoglobulin light chain or transthyretin. Striking differences in the two-dimensional gel proteomes of adipose tissue were observed between controls and patients and between the two types of patients with distinct, additional spots present in the patient specimens that could be assigned as the amyloidogenic proteins in full-length and truncated forms. In patients heterozygotic for transthyretin mutations, wild-type peptides and peptides containing amyloidogenic transthyretin variants were isolated in roughly equal amounts from the same protein spots, indicative of incorporation of both species into the deposits. Furthermore novel spots unrelated to the amyloidogenic proteins appeared in patient samples; some of these were identified as isoforms of serum amyloid P and apolipoprotein E, proteins that have been described previously to be associated with amyloid deposits. Finally changes in the normal expression pattern of resident adipose proteins, such as down-regulation of alphaB-crystallin, peroxiredoxin 6, and aldo-keto reductase I, were observed in apparent association with the presence of amyloid, although their levels did not strictly correlate with the grade of amyloid deposition. This proteomics approach not only provides a way to detect and unambiguously type the deposits in abdominal subcutaneous fat aspirates from patients with amyloidoses but it may also have the capability to generate new insights into the mechanism of the diseases by identifying novel proteins or protein post-translational modifications associated with amyloid infiltration.
Figures






References
-
- Merlini, G., and Bellotti, V. ( 2003) Molecular mechanisms of amyloidosis. N. Engl. J. Med. 349, 583–596 - PubMed
-
- Westermark, P., Benson, M. D., Buxbaum, J. N., Cohen, A. S., Frangione, B., Ikeda, S. I., Masters, C. L., Merlini, G., Saraiva, M. J., and Sipe, J. D. ( 2005) Amyloid: toward terminology clarification—report from the Nomenclature Committee of the International Society of Amyloidosis. Amyloid 12, 1–4 - PubMed
-
- Obici, L., Perfetti, V., Palladini, G., Moratti, R., and Merlini, G. ( 2005) Clinical aspects of systemic amyloid diseases. Biochim. Biophys. Acta 1753, 11–22 - PubMed
-
- Falk, R. H., Comenzo, R. L., and Skinner, M. ( 1997) Medical progress—the systemic amyloidoses. N. Engl. J. Med. 337, 898–909 - PubMed
-
- Picken, M. M. ( 2007) New insights into systemic amyloidosis: the importance of diagnosis of specific type. Curr. Opin. Nephrol. Hypertens. 16, 196–203 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
