

Optic nerve sonography in the diagnostic evaluation of adult brain injury
- PMID: 18477382
- PMCID: PMC2481450
- DOI: 10.1186/cc6897
Optic nerve sonography in the diagnostic evaluation of adult brain injury
Abstract
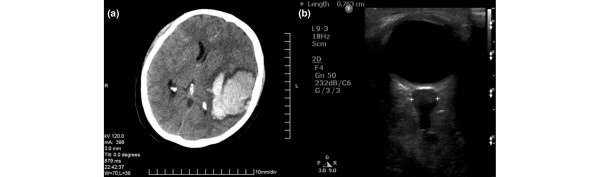
Introduction: The optic nerve sheath diameter (ONSD) may be increased in brain-injured patients, especially children, with intracranial hypertension. We investigated whether measurements of ONSD correlated with simultaneous noninvasive and invasive measurements of the intracranial pressure (ICP) in brain-injured adults.
Methods: Seventy-six critical care patients (58 males; 47 +/- 18 years old) were included in the study. Fifty patients suffered from brain injury, whereas 26 had no intracranial pathology and served as control individuals. Initially, brain-injured patients were evaluated clinically (Glasgow Coma Scale) and using a semiquantitative (I to VI) neuroimaging scale (Marshall Scale). Thereafter, the patients were divided into those with moderate (Marshall Scale = I and Glasgow Coma Scale > 8 [n = 18]) and severe (Marshall Scale = II to VI and Glasgow Coma Scale < or =8 [n = 32]) brain injury. All patients underwent noninvasive measurement of the ICP (estimated ICP) by transcranial Doppler sonography, and synchronous ONSD measurements by optic nerve sonography. Finally, invasive ICP measurement using an intraparenchymal catheter was performed in patients with severe brain injury.
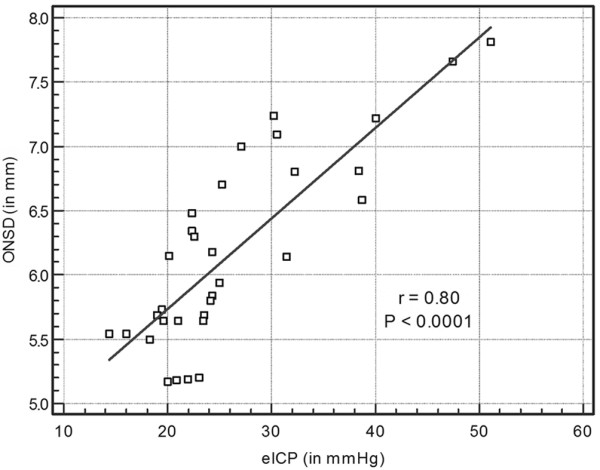
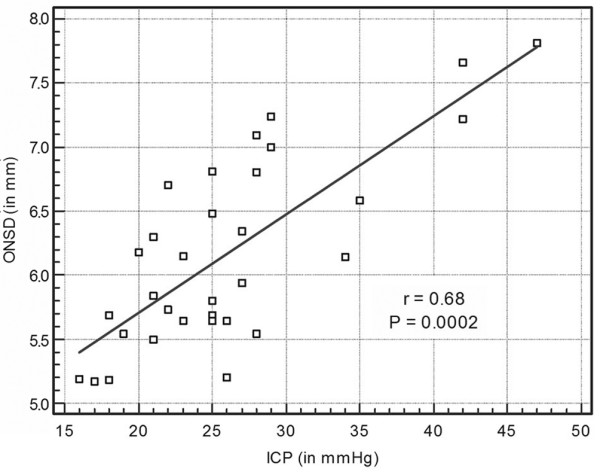
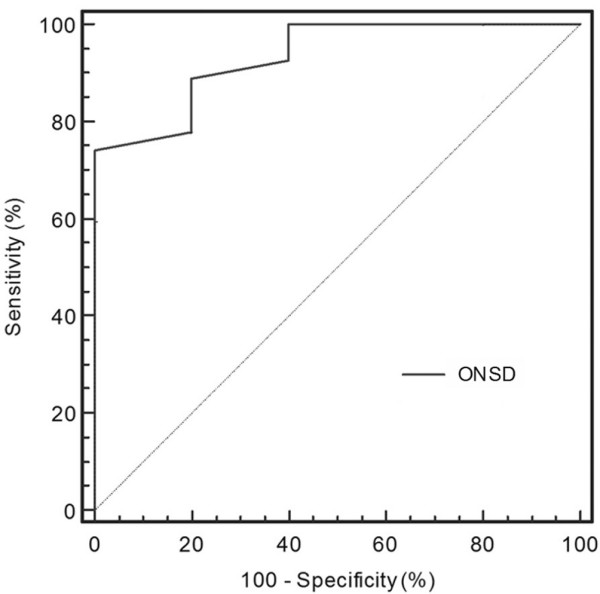
Results: ONSD and estimated ICP were both significantly increased (6.1 +/- 0.7 mm and 26.2 +/- 8.7 mmHg, respectively; P < 0.0001) in patients with severe brain injury as compared with patients with moderate brain injury (4.2 +/- 1.2 mm and 12.0 +/- 3.6 mmHg) and compared with control individuals (3.6 +/- 0.6 mm and 10.3 +/- 3.1 mmHg). Furthermore, in patients with severe brain injury the ONSD measurements were strongly correlated with estimated ICP values (r = 0.80, P < 0.0001) as well as with the neuroimaging scale results (r = 0.82, P < 0.001). In the patients with severe brain injury, ONSD measurements correlated with invasive ICP values (r = 0.68, P = 0.002). The best cut-off value of ONSD for predicting elevated ICP was 5.7 mm (sensitivity = 74.1% and specificity = 100%).
Conclusion: ONSD measurements correlate with noninvasive and invasive measurements of the ICP, and with head computed tomography scan findings in brain-injured adults. Hence, optic nerve sonography may serve as an additional diagnostic tool that could alert clinicians to the presence of elevated ICP, whenever invasive ICP evaluation is contraindicated and/or is not available. This trial is International Standard Randomised Controlled Trial Number registered (ISRCTN 91941687).
Figures
Comment in
-
Ocular sonography in patients with raised intracranial pressure: the papilloedema revisited.Crit Care. 2008;12(3):150. doi: 10.1186/cc6893. Epub 2008 May 16. Crit Care. 2008. PMID: 18495051 Free PMC article.
Similar articles
-
Ultrasonographic evaluation of optic nerve sheath diameter in patients severe traumatic brain injury: a comparison with intraparenchymal pressure monitoring.Neurosurg Rev. 2025 Jan 14;48(1):47. doi: 10.1007/s10143-025-03202-z. Neurosurg Rev. 2025. PMID: 39810071
-
Optic nerve sheath diameter and eyeball transverse diameter in severe head injury and its correlation with intracranial pressure.Clin Neurol Neurosurg. 2024 Jul;242:108310. doi: 10.1016/j.clineuro.2024.108310. Epub 2024 May 8. Clin Neurol Neurosurg. 2024. PMID: 38788542
-
Role of serial ultrasonic optic nerve sheath diameter monitoring in head injury.Neurochirurgie. 2017 Dec;63(6):444-448. doi: 10.1016/j.neuchi.2017.06.001. Epub 2017 Nov 6. Neurochirurgie. 2017. PMID: 29122307
-
Optic nerve sheath diameter: present and future perspectives for neurologists and critical care physicians.Neurol Sci. 2019 Dec;40(12):2447-2457. doi: 10.1007/s10072-019-04015-x. Epub 2019 Jul 31. Neurol Sci. 2019. PMID: 31367861 Review.
-
The Diagnostic Accuracy of Noninvasive Methods to Measure the Intracranial Pressure: A Systematic Review and Meta-analysis.Anesth Analg. 2021 Mar 1;132(3):686-695. doi: 10.1213/ANE.0000000000005189. Anesth Analg. 2021. PMID: 32991330
Cited by
-
Ultrasonography in the emergency department.Crit Care. 2016 Aug 15;20(1):227. doi: 10.1186/s13054-016-1399-x. Crit Care. 2016. PMID: 27523885 Free PMC article. Review.
-
A Review of Glymphatics and the Impact of Osteopathic Manipulative Treatment in Alzheimer's Disease, Concussions, and Beyond.Cureus. 2022 Mar 29;14(3):e23620. doi: 10.7759/cureus.23620. eCollection 2022 Mar. Cureus. 2022. PMID: 35505702 Free PMC article. Review.
-
Intracranial pressure monitoring: Gold standard and recent innovations.World J Clin Cases. 2019 Jul 6;7(13):1535-1553. doi: 10.12998/wjcc.v7.i13.1535. World J Clin Cases. 2019. PMID: 31367614 Free PMC article. Review.
-
Accuracy of Optic Nerve Sheath Diameter Measurements in Pocket-Sized Ultrasound Devices in a Simulation Model.Front Med (Lausanne). 2022 Mar 2;9:831778. doi: 10.3389/fmed.2022.831778. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35308521 Free PMC article.
-
Ultrasound for the anesthesiologists: present and future.ScientificWorldJournal. 2013 Nov 20;2013:683685. doi: 10.1155/2013/683685. ScientificWorldJournal. 2013. PMID: 24348179 Free PMC article. Review.
References
-
- Tayal VS, Neulander M, Norton HJ, Foster T, Saunders T, Blaivas M. Emergency department sonographic measurement of optic nerve sheath diameter to detect findings of increased intracranial pressure in adult head injury patients. Ann Emerg Med. 2007;49:508–514. doi: 10.1016/j.annemergmed.2006.06.040. - DOI - PubMed
-
- Czosnyka M, Matta BF, Smielewski P, Kirkpatrick PJ, Pickard JD. Cerebral perfusion pressure in head-injured patients: a noninvasive assessment using transcranial Doppler ultrasonography. J Neurosurg. 1998;88:802–808. - PubMed
-
- Tsung JW, Blaivas M, Cooper A, Levick NR. A rapid noninvasive method of detecting elevated intracranial pressure using bedside ocular ultrasound: application to 3 cases of head trauma in the pediatric emergency department. Pediatr Emerg Care. 2005;21:94–98. doi: 10.1097/01.pec.0000159052.64930.64. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
