

Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer
- PMID: 18477782
- PMCID: PMC2718688
- DOI: 10.1001/jama.299.18.2151
Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer
Erratum in
- JAMA. 2010 Apr 21;303(15):1482
Abstract
Context: Screening ultrasound may depict small, node-negative breast cancers not seen on mammography.
Objective: To compare the diagnostic yield, defined as the proportion of women with positive screen test results and positive reference standard, and performance of screening with ultrasound plus mammography vs mammography alone in women at elevated risk of breast cancer.
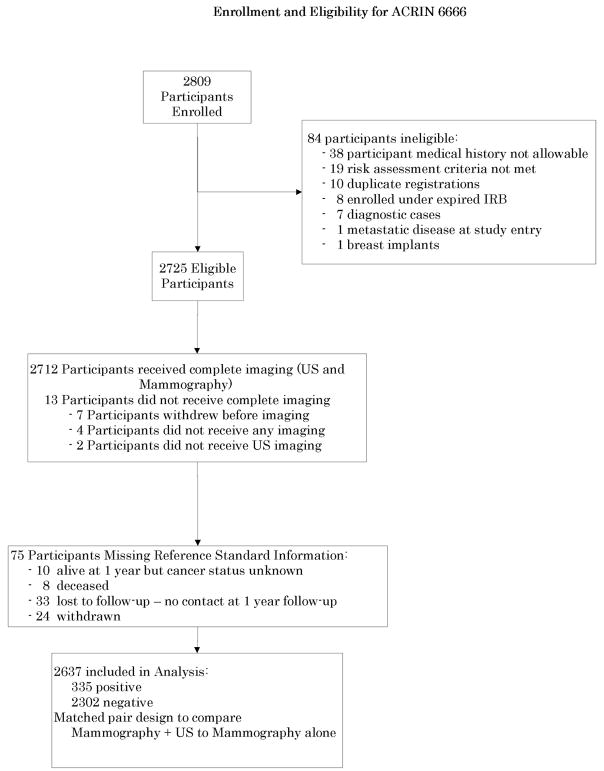
Design, setting, and participants: From April 2004 to February 2006, 2809 women, with at least heterogeneously dense breast tissue in at least 1 quadrant, were recruited from 21 sites to undergo mammographic and physician-performed ultrasonographic examinations in randomized order by a radiologist masked to the other examination results. Reference standard was defined as a combination of pathology and 12-month follow-up and was available for 2637 (96.8%) of the 2725 eligible participants.
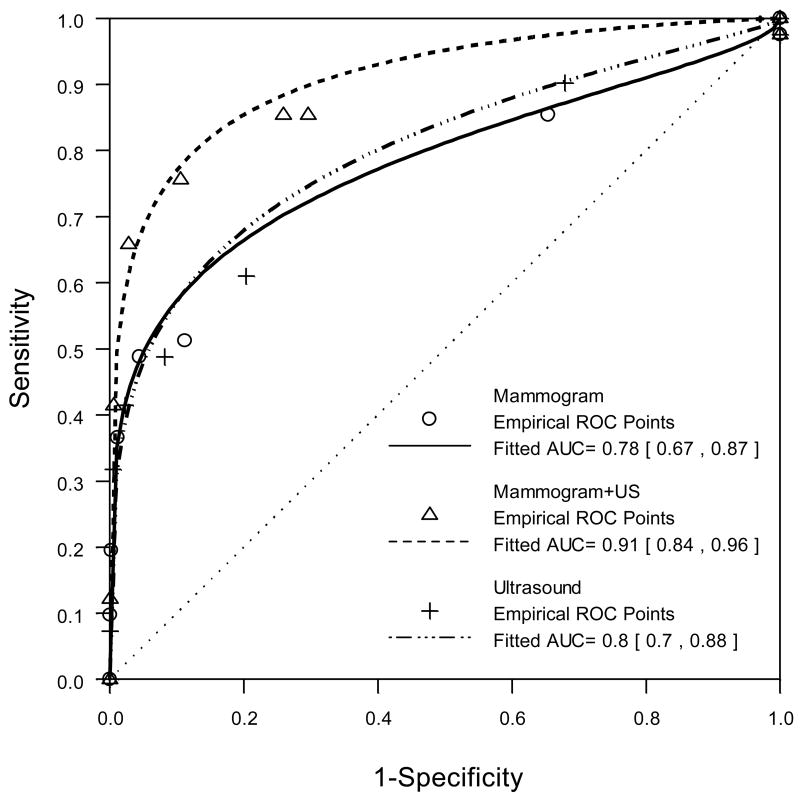
Main outcome measures: Diagnostic yield, sensitivity, specificity, and diagnostic accuracy (assessed by the area under the receiver operating characteristic curve) of combined mammography plus ultrasound vs mammography alone and the positive predictive value of biopsy recommendations for mammography plus ultrasound vs mammography alone.
Results: Forty participants (41 breasts) were diagnosed with cancer: 8 suspicious on both ultrasound and mammography, 12 on ultrasound alone, 12 on mammography alone, and 8 participants (9 breasts) on neither. The diagnostic yield for mammography was 7.6 per 1000 women screened (20 of 2637) and increased to 11.8 per 1000 (31 of 2637) for combined mammography plus ultrasound; the supplemental yield was 4.2 per 1000 women screened (95% confidence interval [CI], 1.1-7.2 per 1000; P = .003 that supplemental yield is 0). The diagnostic accuracy for mammography was 0.78 (95% CI, 0.67-0.87) and increased to 0.91 (95% CI, 0.84-0.96) for mammography plus ultrasound (P = .003 that difference is 0). Of 12 supplemental cancers detected by ultrasound alone, 11 (92%) were invasive with a median size of 10 mm (range, 5-40 mm; mean [SE], 12.6 [3.0] mm) and 8 of the 9 lesions (89%) reported had negative nodes. The positive predictive value of biopsy recommendation after full diagnostic workup was 19 of 84 for mammography (22.6%; 95% CI, 14.2%-33%), 21 of 235 for ultrasound (8.9%, 95% CI, 5.6%-13.3%), and 31 of 276 for combined mammography plus ultrasound (11.2%; 95% CI. 7.8%-15.6%).
Conclusions: Adding a single screening ultrasound to mammography will yield an additional 1.1 to 7.2 cancers per 1000 high-risk women, but it will also substantially increase the number of false positives.
Trial registration: clinicaltrials.gov Identifier: NCT00072501.
Figures
Comment in
-
The "coming of age" of nonmammographic screening for breast cancer.JAMA. 2008 May 14;299(18):2203-5. doi: 10.1001/jama.299.18.2203. JAMA. 2008. PMID: 18477789 No abstract available.
-
[Screening ultrasound of breast cancer in a high-risk population].J Radiol. 2008 Jun;89(6):748. doi: 10.1016/s0221-0363(08)73780-6. J Radiol. 2008. PMID: 18641561 French. No abstract available.
-
Is mammography + ultrasound better than mammography alone for high-risk women?J Fam Pract. 2008 Aug;57(8):508. J Fam Pract. 2008. PMID: 18697289 No abstract available.
-
Ultrasound and mammography for breast cancer screening.JAMA. 2008 Oct 1;300(13):1514-5; author reply 1515. doi: 10.1001/jama.300.13.1514-b. JAMA. 2008. PMID: 18827203 No abstract available.
-
Ultrasound and mammography for breast cancer screening.JAMA. 2008 Oct 1;300(13):1514; author reply 1515. doi: 10.1001/jama.300.13.1514-a. JAMA. 2008. PMID: 18827204 No abstract available.
-
Ultrasound for the screening of breast cancer.Curr Oncol Rep. 2008 Nov;10(6):527-8. doi: 10.1007/s11912-008-0079-7. Curr Oncol Rep. 2008. PMID: 18928668 No abstract available.
References
-
- Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002 Sep 3;137(5 Part 1):347–360. - PubMed
-
- Tabar L, Vitak B, Chen HH, et al. The Swedish Two-County Trial twenty years later. Updated mortality results and new insights from long-term follow-up. Radiol Clin North Am. 2000;38(4):625–651. - PubMed
-
- Smith RA, Duffy SW, Gabe R, Tabar L, Yen AM, Chen TH. The randomized trials of breast cancer screening: what have we learned? Radiol Clin North Am. 2004 Sep;42(5):793–806. v. - PubMed
-
- Tabar L, Tot T, Dean PB. Early detection of breast cancer: Large-section and subgross thick-section histologic correlation with mammographic appearances. Radiographics. 2007;27:S5–S35.
-
- Stomper PC, D’Souza DJ, DiNitto PA, Arredondo MA. Analysis of parenchymal density on mammograms in 1353 women 25–79 years old. AJR Am J Roentgenol. 1996 Nov;167(5):1261–1265. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
