

Preventive antibacterial therapy in acute ischemic stroke: a randomized controlled trial
- PMID: 18478129
- PMCID: PMC2373885
- DOI: 10.1371/journal.pone.0002158
Preventive antibacterial therapy in acute ischemic stroke: a randomized controlled trial
Abstract
Background: Pneumonia is a major risk factor of death after acute stroke. In a mouse model, preventive antibacterial therapy with moxifloxacin not only prevents the development of post-stroke infections, it also reduces mortality, and improves neurological outcome significantly. In this study we investigate whether this approach is effective in stroke patients.
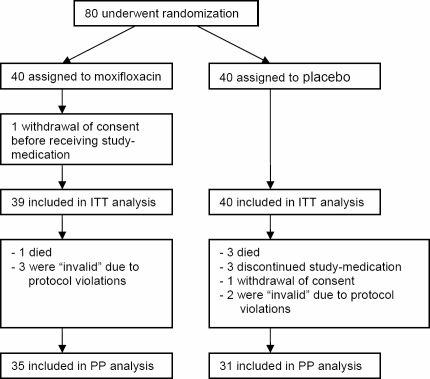
Methods: Preventive ANtibacterial THERapy in acute Ischemic Stroke (PANTHERIS) is a randomized, double-blind, placebo-controlled trial in 80 patients with severe, non-lacunar, ischemic stroke (NIHSS>11) in the middle cerebral artery (MCA) territory. Patients received either intravenous moxifloxacin (400 mg daily) or placebo for 5 days starting within 36 hours after stroke onset. Primary endpoint was infection within 11 days. Secondary endpoints included neurological outcome, survival, development of stroke-induced immunodepression, and induction of bacterial resistance.
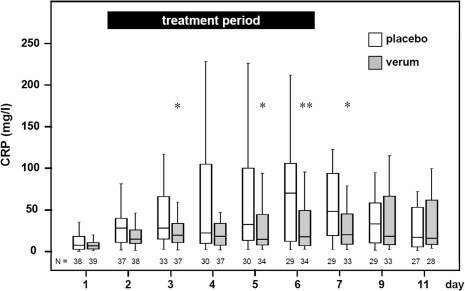
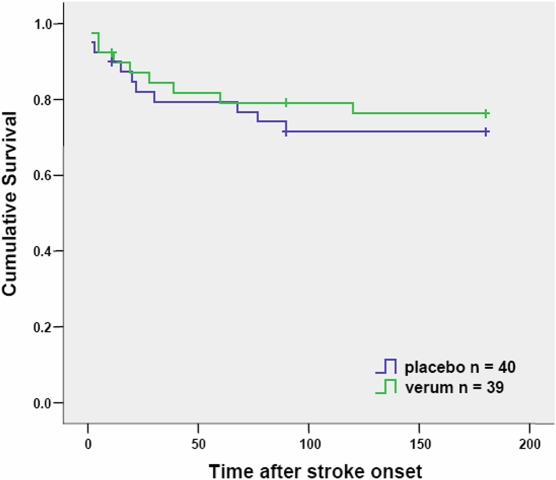
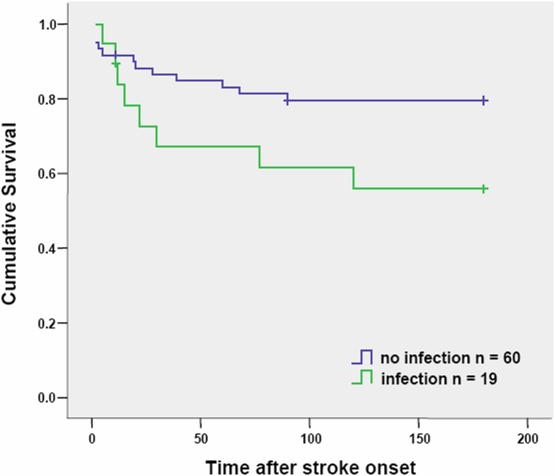
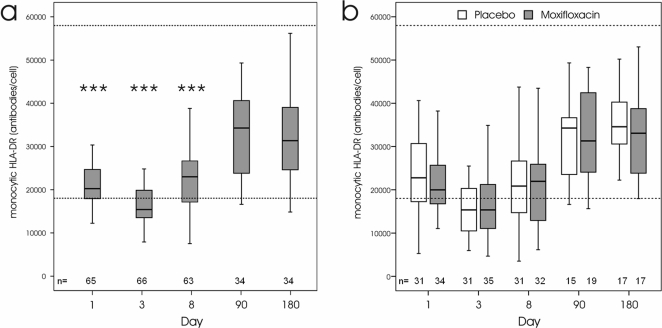
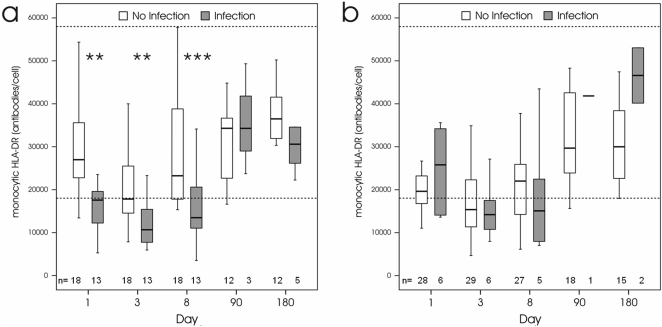
Findings: On intention-to treat analysis (79 patients), the infection rate at day 11 in the moxifloxacin treated group was 15.4% compared to 32.5% in the placebo treated group (p = 0.114). On per protocol analysis (n = 66), moxifloxacin significantly reduced infection rate from 41.9% to 17.1% (p = 0.032). Stroke associated infections were associated with a lower survival rate. In this study, neurological outcome and survival were not significantly influenced by treatment with moxifloxacin. Frequency of fluoroquinolone resistance in both treatment groups did not differ. On logistic regression analysis, treatment arm as well as the interaction between treatment arm and monocytic HLA-DR expression (a marker for immunodepression) at day 1 after stroke onset was independently and highly predictive for post-stroke infections.
Interpretation: PANTHERIS suggests that preventive administration of moxifloxacin is superior in reducing infections after severe non-lacunar ischemic stroke compared to placebo. In addition, the results emphasize the pivotal role of immunodepression in developing post-stroke infections.
Trial registration: Controlled-Trials.com ISRCTN74386719.
Conflict of interest statement
Figures
References
-
- Davenport RJ, Dennis MS, Wellwood I, Warlow CP. Complications after acute stroke. Stroke. 1996;27:415–20. - PubMed
-
- Johnston KC, Li JY, Lyden PD, Hanson SK, Feasby TE, et al. Medical and neurological complications of ischemic stroke: experience from the RANTTAS trial. RANTTAS investigators. Stroke; 1998;29:447–53. - PubMed
-
- Meisel C, Schwab JM, Prass K, Meisel A, Dirnagl U. Central nervous system injury-induced immunedeficiency syndrome. Nat Rev Neurosci. 2005;6:775–86. - PubMed
-
- Langhorne P, Scott DJ, Robertson L, MacDonald J, Jones L, et al. Medical complications after stroke: a multicenter study. Stroke. 2000;31:1223–29. - PubMed
-
- Katzan IL, Cebul RD, Husak SH, Dawson NV, Baker DW. The effect of pneumonia on mortality among patients hospitalized for acute stroke. Neurology. 2003;60:620–25. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
