

The physical state of HPV16 infection and its clinical significance in cancer precursor lesion and cervical carcinoma
- PMID: 18478264
- PMCID: PMC12161717
- DOI: 10.1007/s00432-008-0413-3
The physical state of HPV16 infection and its clinical significance in cancer precursor lesion and cervical carcinoma
Erratum in
-
Correction to: The physical state of HPV16 infection and its clinical significance in cancer precursor lesion and cervical carcinoma.J Cancer Res Clin Oncol. 2020 May;146(5):1377. doi: 10.1007/s00432-020-03164-3. J Cancer Res Clin Oncol. 2020. PMID: 32157436 Free PMC article.
Abstract
Purpose: Integration of high-risk human papillomavirus (HR-HPVs) into the host DNA has been proposed as a risk for cervical carcinogenesis. HPV-16 is the predominant high-risk type and its integration ration varied largely in different cervical cancer (CC) samples. The aim of this study was to evaluate the correlation between physical state of HPV16 infection and extent of cervical lesion, as well as the clinical significance of virus existing state.
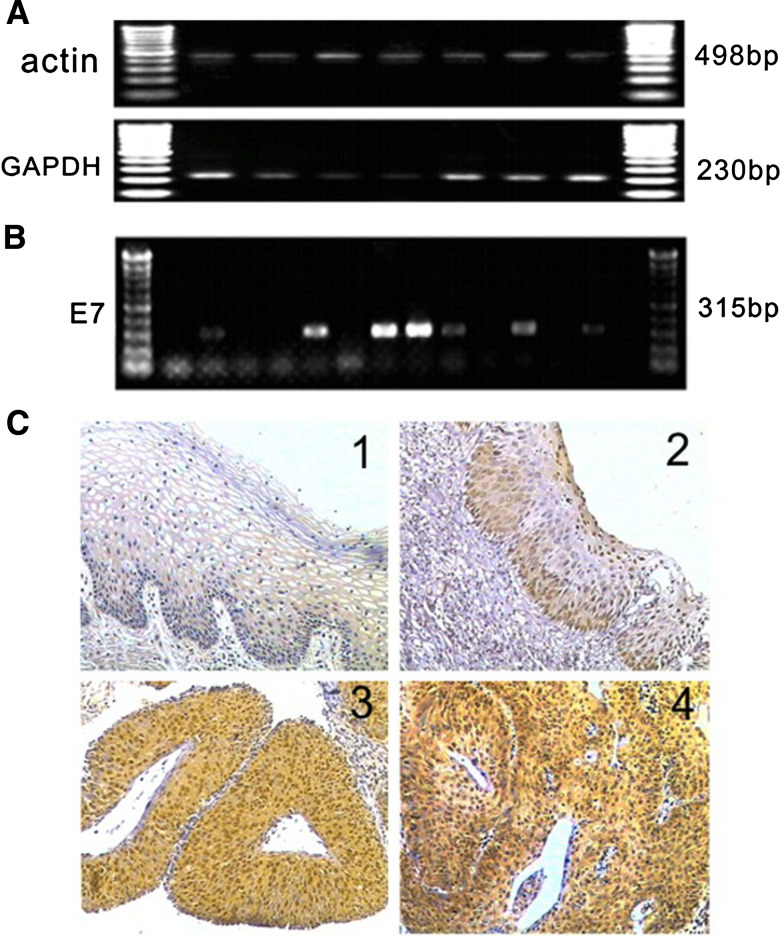
Methods: A total of 252 cases of paraffin-embedded blocks derived from cancer precursor lesion and cervical carcinoma samples were detected by HC-II for HR-HPV infection. HPV16 infection was confirmed by PCR and immunohistochemistry for HPV16 E7 simultaneously. The physical state of HPV16 infection were assessed by PCR for 3 overlapping fragments in E2 gene and multiple PCR for E2 gene and E7 gene.
Results: The infection ratio of HR-HPV in normal cervical tissue, cervical intraepithelial neoplasia (CIN) I, CIN II, CIN III and cervical cancer were 15.0, 32.8, 54.3, 69.7, 93.8%, respectively. HR-HPV positive samples of 62.8% were infected with HPV16. The integration ratio of HPV16 in CIN III and cervical carcinoma were 35.7 and 58.1% respectively, both of which were significantly higher than that of CIN I and normal cervical tissues. The discrepancy was statistically significant (P < 0.05). Furthermore, it was observed that persistent virus infection and progression of cervical lesion were more common in CIN I with integrated HPV16 than that with episomal HPV16.
Conclusion: The integration ratio of HPV16 was accompanied by an increase in the grade of cervical lesion. The integrated state of HPV16 infection was strongly associated with persistent HPV infection and progression of cervical lesions.
Figures

References
-
- Bosch FX, Manos MM, Munoz N, Sherman M, Jansen AM, Peto J, Schiffman MH, Moreno V, Kurman R, Shah KV (1995) Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst 87:796–802 - DOI - PubMed
