

Adverse outcomes following hospitalization in acutely ill older patients
- PMID: 18479512
- PMCID: PMC2391142
- DOI: 10.1186/1471-2318-8-10
Adverse outcomes following hospitalization in acutely ill older patients
Abstract
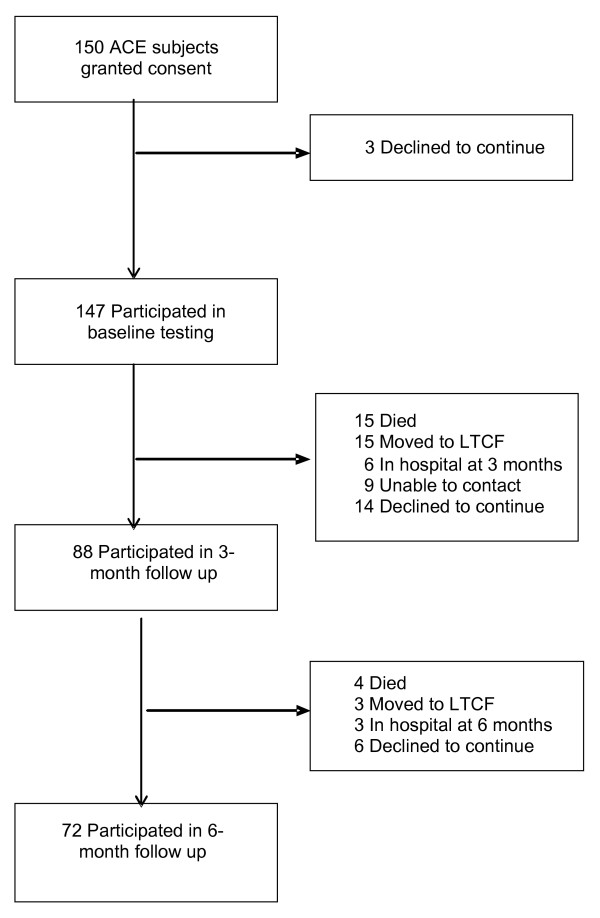
Background: The longitudinal outcomes of patients admitted to acute care for elders units (ACE) are mixed. We studied the associations between socio-demographic and functional measures with hospital length of stay (LOS), and which variables predicted adverse events (non-independent living, readmission, death) 3 and 6 months later.
Methods: Prospective cohort study of community-living, medical patients age 75 or over admitted to ACE at a teaching hospital.
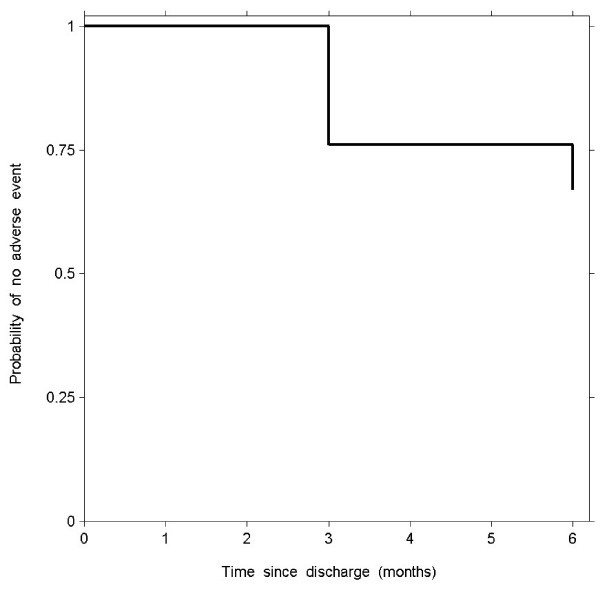
Results: The population included 147 subjects, median LOS of 9 days (interquartile range 5-15 days). All returned home/community after hospitalization. Just prior to discharge, baseline timed up and go test (TUG, P < 0.001), bipedal stance balance (P = 0.001), and clinical frailty scale scores (P = 0.02) predicted LOS, with TUG as the only independent predictor (P < 0.001) in multiple regression analysis. By 3 months, 59.9% of subjects remained free of an adverse event, and by 6 months, 49.0% were event free. The 3 and 6-month mortality was 10.2% and 12.9% respectively. Almost one-third of subjects had developed an adverse event by 6 months, with the highest risk within the first 3 months post discharge. An abnormal TUG score was associated with increased adjusted hazard ratio [HR] 1.28, 95% confidence interval [CI] 1.03 to 1.59, P = 0.03. A higher FMMSE score (adjusted HR 0.89, 95% CI 0.82 to 0.96, P = 0.003) and independent living before hospitalization (adjusted HR 0.42, 95% CI 0.21 to 0.84, P = 0.01) were associated with reduced risk of adverse outcome.
Conclusion: Some ACE patients demonstrate further functional decline following hospitalization, resulting in loss of independence, repeat hospitalization, or death. Abnormal TUG is associated with prolonged LOS and future adverse outcomes.
Figures
References
-
- Palmer RM, Landefeld CS, Kresevic DM, Kowal J. A medical unit for the acute care of the elderly. J Am Geriatr Soc. 1994;42:545–52. - PubMed
-
- Covinsky KE, Palmer RM, Kresevic DM, Kahana E, Counsell SR, Fortinsky RH, Landefeld CS. Improving functional outcomes in older patients: lessons from an acute care for elders unit. Jt Comm J Qual Improv. 1998;24:63–76. - PubMed
-
- Covinsky KE, King JT, Jr, Quinn LM, Siddique R, Palmer R, Kresevic DM, Fortinsky RH, Kowal J, Landefeld CS. Do acute care for elders units increase hospital costs? A cost analysis using the hospital perspective. J Am Geriatr Soc. 1997;45:729–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
