

Tibial artery calcification as a marker of amputation risk in patients with peripheral arterial disease
- PMID: 18482666
- PMCID: PMC2836514
- DOI: 10.1016/j.jacc.2007.12.058
Tibial artery calcification as a marker of amputation risk in patients with peripheral arterial disease
Abstract
Objectives: The purpose of this study was to evaluate the relationship between calcification in tibial arteries, the degree of limb ischemia, and the near-term risk of amputation.
Background: Determining the amputation risk in patients with peripheral arterial disease (PAD) remains difficult. Developing new measures to identify patients who are at high risk for amputation would allow for targeted interventions and focused trials aimed at limb preservation.
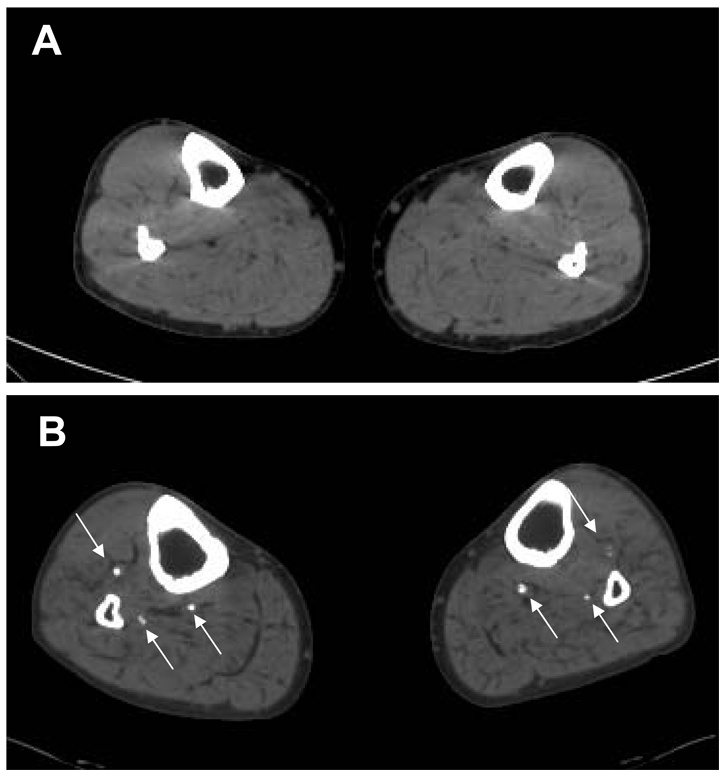
Methods: Two hundred twenty-nine patients underwent evaluation by history, arterial Doppler, and multislice computed tomography of the lower extremities. We then explored the relationship between a tibial artery calcification (TAC), traditional risk factors for PAD, limb status at presentation, and near-term amputation risk.
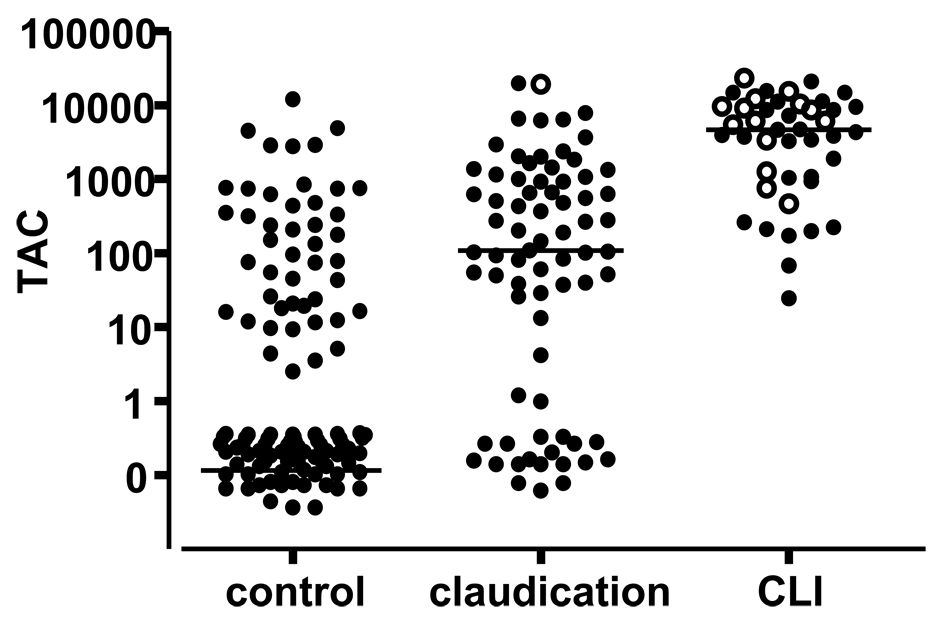
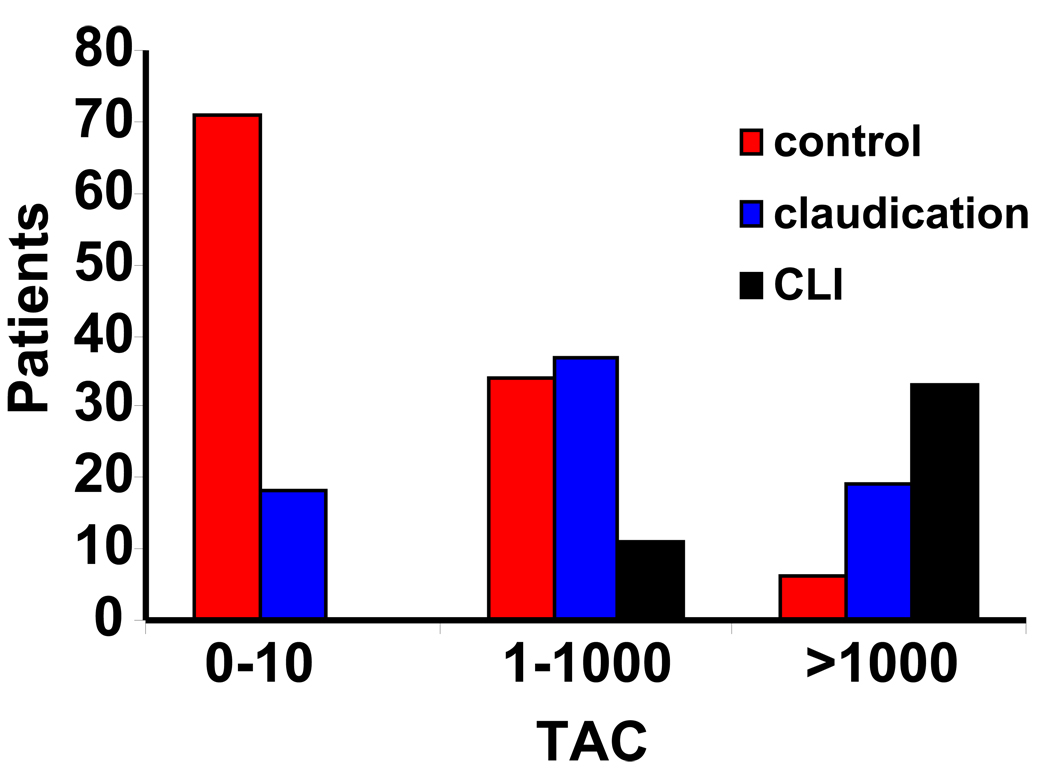
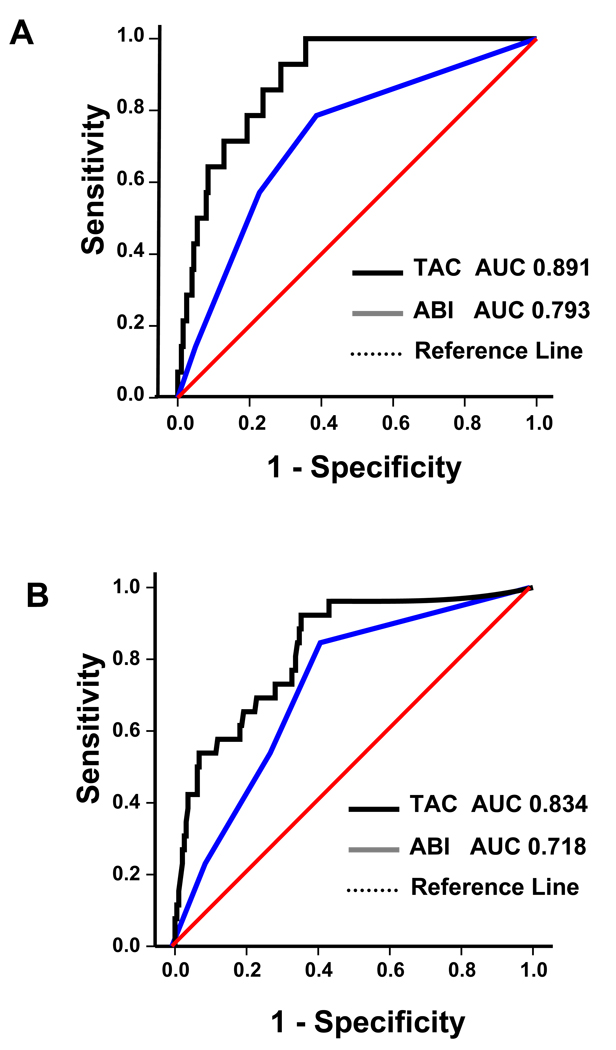
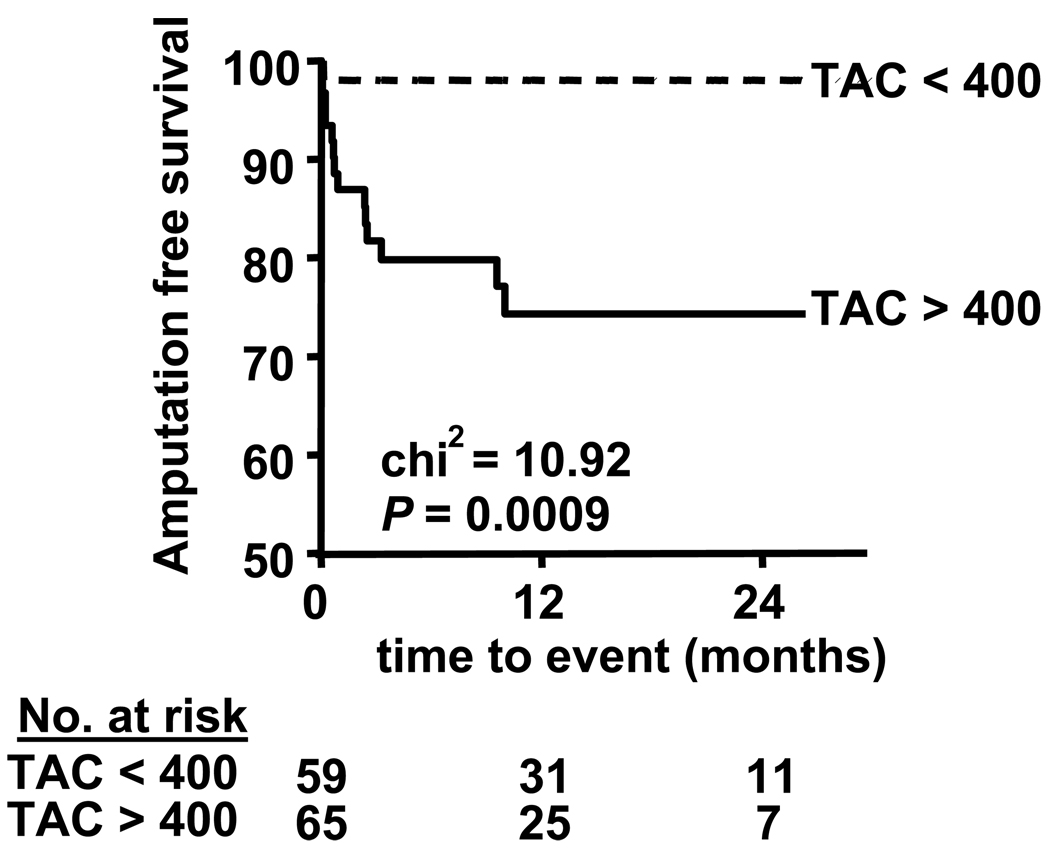
Results: Increased age and traditional atherosclerosis risk factors were associated with higher TAC scores. Patients with critical limb ischemia had the highest TAC scores, and increasing TAC scores were associated with worsening levels of limb ischemia in ordinal regression analysis. Receiver-operator characteristic analysis suggested that the TAC score predicted amputation better than the ankle-brachial index (ABI). Symptomatic patients with a TAC score greater than 400 had a significantly increased risk of amputation. In Cox regression analysis, there was a strong association between the TAC score and the risk of major amputation that remained after adjustment for traditional risk factors and the ABI.
Conclusions: In patients presenting with PAD, the TAC score is associated with the stage of disease and it identifies those who are at high risk for amputation better than traditional risk factors and an abnormal ABI.
Conflict of interest statement
Figures
Comment in
-
Footnotes on critical limb ischemia.J Am Coll Cardiol. 2008 May 20;51(20):1975-6. doi: 10.1016/j.jacc.2008.02.041. J Am Coll Cardiol. 2008. PMID: 18482667 No abstract available.
References
-
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999– 2000. Circulation. 2004;110:738–743. - PubMed
-
- Izquierdo-Porrera AM, Gardner AW, Bradham DD, et al. Relationship between objective measures of peripheral arterial disease severity to self-reported quality of life in older adults with intermittent claudication. J Vasc Surg. 2005;41:625–630. - PubMed
-
- Long J, Modrall JG, Parker BJ, Swann A, Welborn MB, 3rd, Anthony T. Correlation between ankle-brachial index, symptoms, and health-related quality of life in patients with peripheral vascular disease. J Vasc Surg. 2004;39:723–727. - PubMed
-
- Feringa HH, Bax JJ, van Waning VH, et al. The long-term prognostic value of the resting and postexercise ankle-brachial index. Arch Intern Med. 2006;166:529–535. - PubMed
-
- Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med. 1992;326:381–386. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
