

Level of arterial ligation in rectal cancer surgery: low tie preferred over high tie. A review
- PMID: 18483828
- PMCID: PMC2468314
- DOI: 10.1007/s10350-008-9328-y
Level of arterial ligation in rectal cancer surgery: low tie preferred over high tie. A review
Abstract
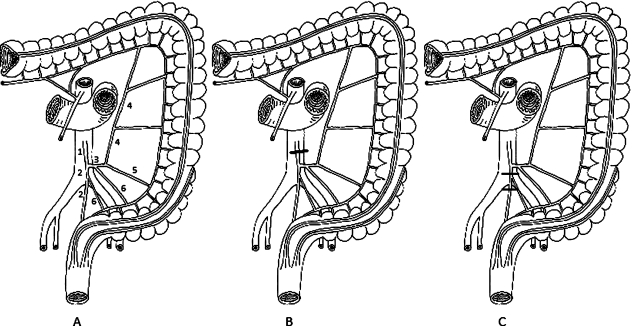
Consensus does not exist on the level of arterial ligation in rectal cancer surgery. From oncologic considerations, many surgeons apply high tie arterial ligation (level of inferior mesenteric artery). Other strategies include ligation at the level of the superior rectal artery, just caudally to the origin of the left colic artery (low tie), and ligation at a level without any intraoperative definition of the inferior mesenteric or superior rectal arteries. Publications concerning the level of ligation in rectal cancer surgery were systematically reviewed. Twenty-three articles that evaluated oncologic outcome (n = 14), anastomotic circulation (n = 5), autonomous innervation (n = 5), and tension on the anastomosis/anastomotic leakage (n = 2) matched our selection criteria and were systematically reviewed. There is insufficient evidence to support high tie as the technique of choice. Furthermore, high tie has been proven to decrease perfusion and innervation of the proximal limb. It is concluded that neither the high tie strategy nor the low tie strategy is evidence based and that low tie is anatomically less invasive with respect to circulation and autonomous innervation of the proximal limb of anastomosis. As a consequence, in rectal cancer surgery low tie should be the preferred method.
Figures
References
-
- Moynihan BG. The surgical treatment of cancer of the sigmoid flexure and rectum. Surg Gynecol Obstet 1908;463.
-
- Ault GW, Castro AF, Smith RS. Clinical study of ligation of the inferior mesenteric artery in left colon resections. Surg Gynecol Obstet. 1952;94:223–228. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous