

Evaluation of structure-function relationships in asthma using multidetector CT and hyperpolarized He-3 MRI
- PMID: 18486011
- PMCID: PMC2744977
- DOI: 10.1016/j.acra.2007.10.019
Evaluation of structure-function relationships in asthma using multidetector CT and hyperpolarized He-3 MRI
Abstract
Rationale and objectives: Although multiple detector computed tomography (MDCT) and hyperpolarized gas magnetic resonance imaging (HP MRI) have demonstrated ability to detect structural and ventilation abnormalities in asthma, few studies have sought to exploit or cross-validate the regional information provided by these techniques. The purpose of this work is to assess regional disease in asthma by evaluating the association of sites of ventilation defect on HP MRI with other regional markers of airway disease, including air trapping on MDCT and inflammatory markers on bronchoscopy.
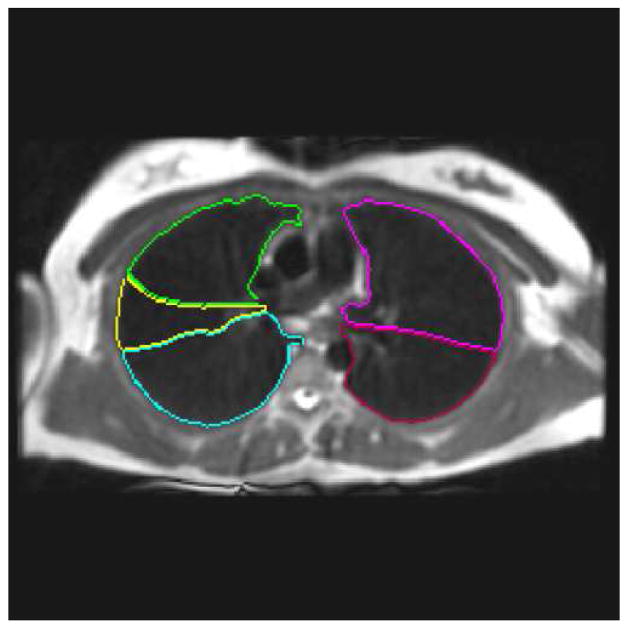
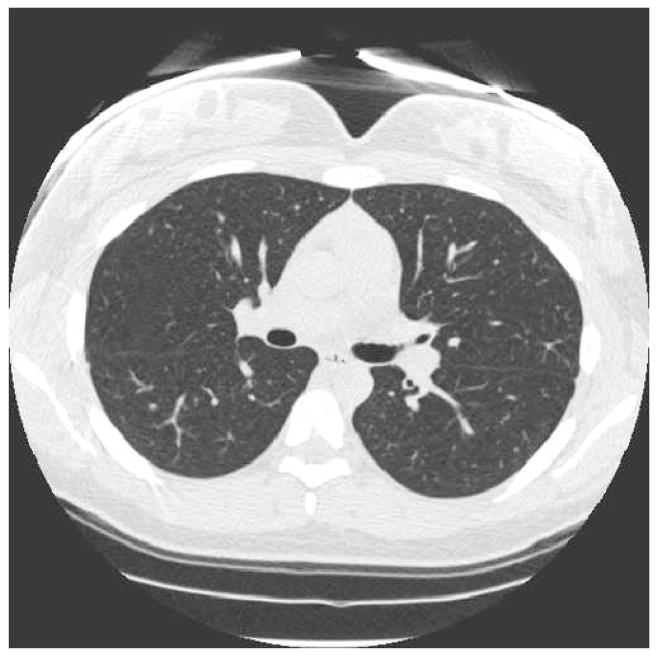
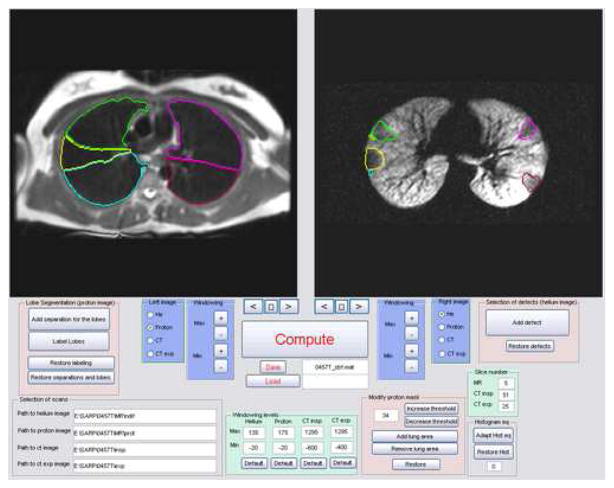
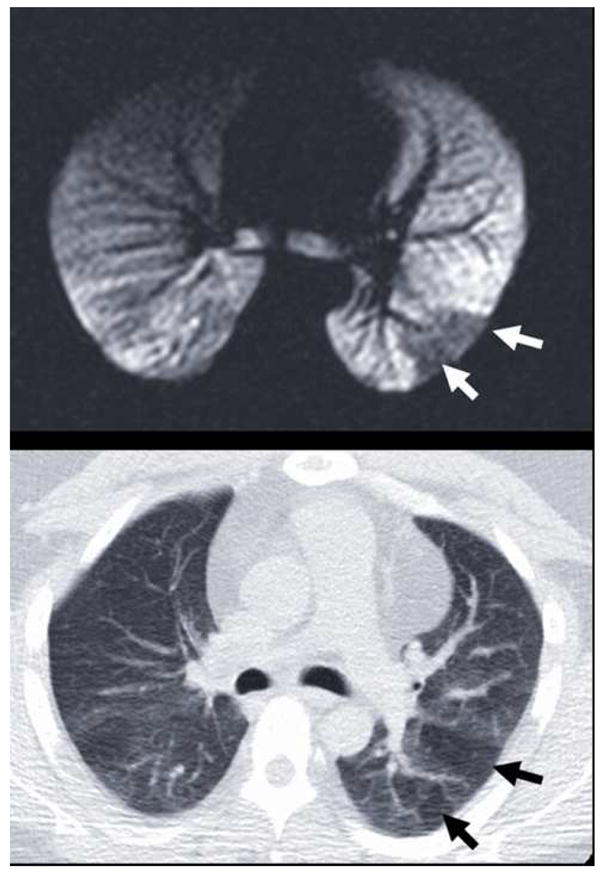
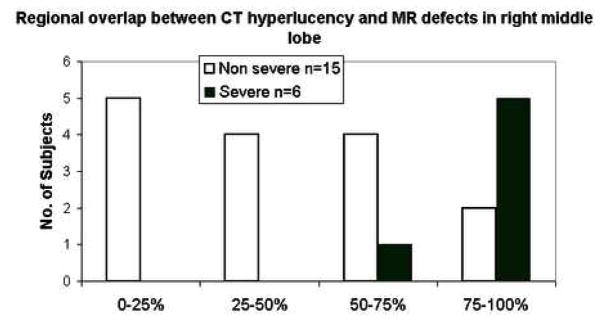
Materials and methods: Both HP MRI using helium-3 and MDCT were acquired in the same patients. Supervised segmentation of the lung lobes on MRI and MDCT facilitated regional comparisons of ventilation abnormalities in the lung parenchyma. The percentage of spatial overlap was evaluated between regions of ventilation defect on HP MRI and hyperlucency on MDCT to determine associations between obstruction and likely regions of gas trapping. Similarly, lung lobes with high defect volume were compared to lobes with low defect volume for differences in inflammatory cell number and percentage using bronchoscopic assessment.
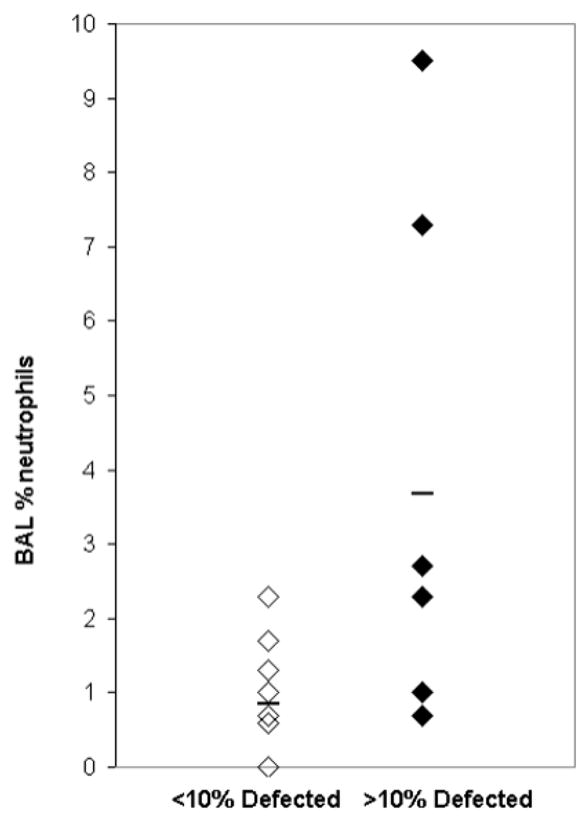
Results: There was significant overlap between sites of ventilation defect on HP MRI and hyperlucency on MDCT suggesting that sites of airway obstruction and air trapping are associated in asthma. The percent (r=0.68; P= .0039) and absolute (r=0.61; P= .0125) number of neutrophils on bronchoalveolar lavage for the sampled lung lobe also directly correlated with increased defect volume.
Conclusions: These results show promise for using image guidance to assess specific regions of ventilation defect or air trapping in heterogeneous obstructive lung diseases such as asthma.
Figures
References
-
- Hartert TV, Peebles RS., Jr Epidemiology of asthma: the year in review. Curr Opin Pulm Med. 2000;6(1):4–9. - PubMed
-
- Sears MR, Greene JM, Willan AR, Wiecek EM, Taylor DR, Flannery EM, Cowan JO, Herbison GP, Silva PA, Poulton R. A Longitudinal, Population-Based, Cohort Study of Childhood Asthma Followed to Adulthood. The New England Journal of Medicine. 2003;349:1414–1422. - PubMed
-
- Postma DS, Timens W. Remodeling in asthma and chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(5):434–439. - PubMed
-
- Permutt S. Current status of functional pulmonary imaging. Acad Radiol. 2005;12(11):1359–1361. - PubMed
-
- Haczku A, Emami K, Fischer MC, Kadlecek S, Ishii M, Panettieri RA, Rizi RR. Hyperpolarized 3He MRI in asthma measurements of regional ventilation following allergic sensitization and challenge in mice--preliminary results. Acad Radiol. 2005;12(11):1362–1370. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
