

Review
doi: 10.1016/j.pop.2008.01.007.
Disorders involving calcium, phosphorus, and magnesium
Affiliations
- PMID: 18486714
- PMCID: PMC2486454
- DOI: 10.1016/j.pop.2008.01.007
Item in Clipboard
Review
Disorders involving calcium, phosphorus, and magnesium
Prim Care.
2008 Jun.
Abstract
Disorders of mineral metabolism are common in both the office and hospital setting. The diagnosis can be simplified by remembering the target organs involved--intestine, kidney, and bone--and by assessing the presence of kidney disease, levels of parathyroid hormone, and vitamin D status. Although the list of possible causes for these derangements is long, most patients who have hypercalcemia have hyperparathyroidism or malignancy; those who have hypocalcemia, hypophosphatemia, and hypomagnesemia have reduced gastrointestinal absorption, and those who have hyperphosphatemia and hypermagnesemia have increased intake in the setting of kidney disease.
Figures
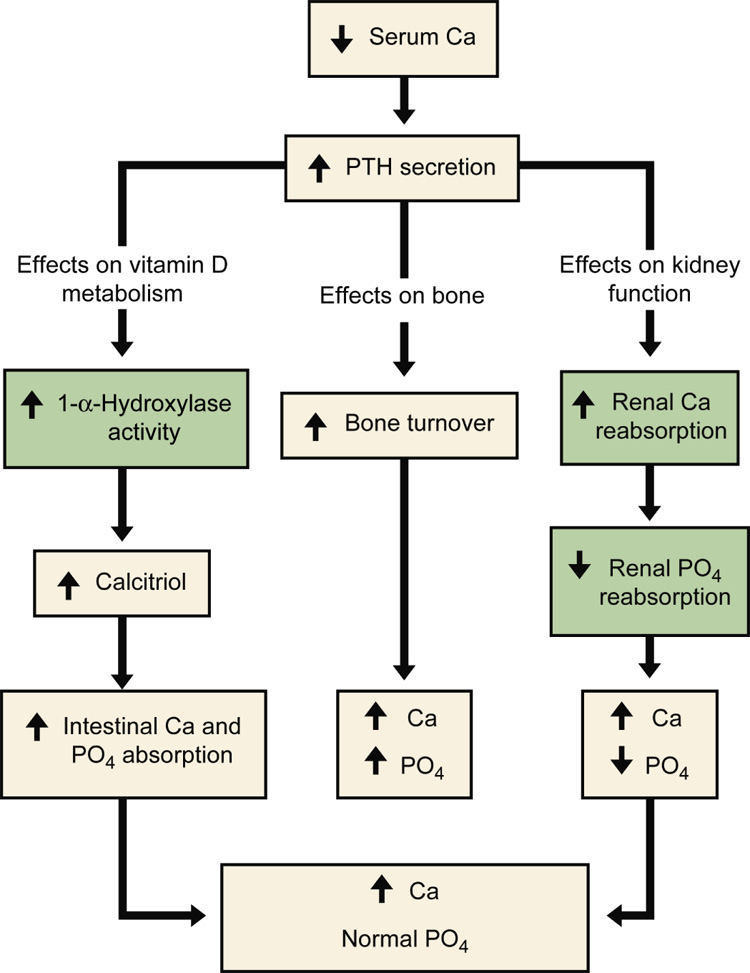
Normal homeostatic response to hypocalcemia. In the presence of hypocalcemia, parathyroid hormone (PTH) secretion is increased. PTH acts on three target organs. PTH works level at the intestine indirectly by first increasing the 1-α-hydroxalase activity in the kidney. This enzyme converts calcidiol to calcitriol, which then increases intestinal absorption of both calcium and phosphorus. In bone, parathyroid hormone increases bone turnover, resulting in a release of calcium and phosphorus from bone. Lastly, PTH works directly on the kidney to increase renal calcium reabsorption and decrease renal phosphorus reabsorption. The net effect is a rise in serum calcium but no net change in serum phosphorus. The gray boxes indicate homeostatic steps in the kidney that are impaired in the setting of kidney disease. From Moe SM, Sprague S: Mineral Bone Disorders in Chronic Kidney Disease. In Brenner B (ed): The Kidney, 8th ed. Philadelphia: Saunders, 2008, Vol 2, p 1784 with permission.
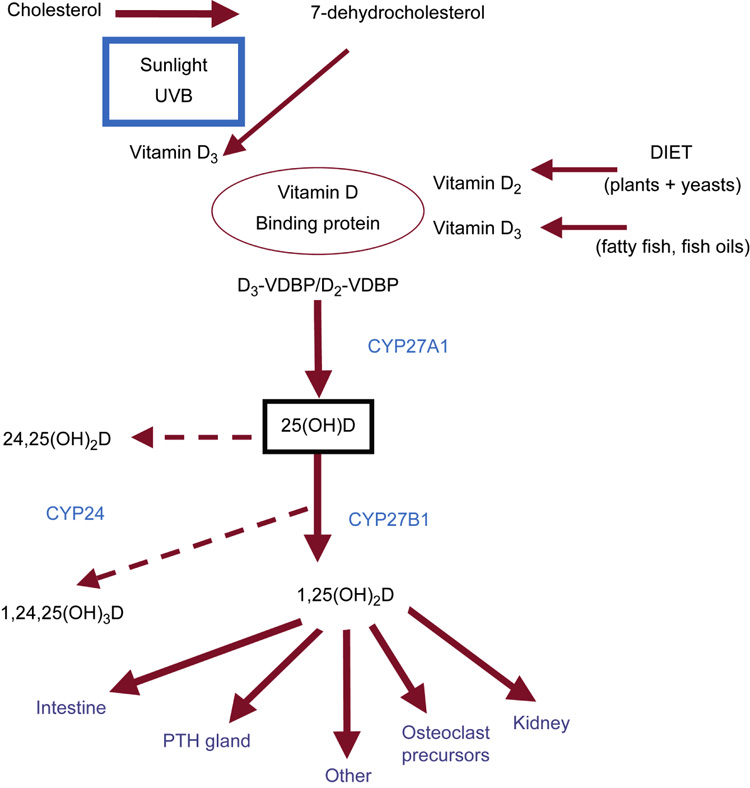
Overview of vitamin D metabolism. Vitamin D is obtained from dietary sources, and is metabolized via ultraviolet light from 7-DHC in the skin. Both sources (diet and skin) of Vitamin D2 and vitamin D3 bind to vitamin D binding protein (VDBP) and circulate to the liver. In the liver, vitamin D is hydroxylated by CYP27A1 to 25(OH)D, commonly referred to as calcidiol. Calcidiol is then further metabolized to calcitriol by the 1-α-hydroxylase enzyme (CYP27B1) at the level of the kidney. The active metabolite 1,25(OH)2D (calcitriol) acts principally on the target organs of intestine, parathyroid (PTH) gland, bone cell precursors, and the kidney. Calcitriol is metabolized to the inert 1,24,25(OH)3D through the action of the 24,25-hydroxylase enzyme (CYP24). Calcidiol is similarly hydroxylated to 24,25(OH)2D. From Moe SM, Sprague S: Mineral Bone Disorders in Chronic Kidney Disease. In Brenner B (ed): The Kidney, 8th ed. Philadelphia: Saunders, 2008, Vol 2, p 1784 with permission.
References
-
- Barbagallo M, Dominguez LJ. Magnesium metabolism in type 2 diabetes mellitus, metabolic syndrome and insulin resistance. Arch Biochem Biophys. 2007;458:40. - PubMed
-
- Beasley R, Aldington S. Magnesium in the treatment of asthma. Curr Opin Allergy Clin Immunol. 2007;7:107. - PubMed
-
- Bilezikian JP, Potts JT, Jr, Fuleihan Gel H, et al. Summary statement from a workshop on asymptomatic primary hyperparathyroidism: a perspective for the 21st century. J Bone Miner Res. 2002;17(Suppl 2):N2. - PubMed
-
- Bilezikian JP, Silverberg SJ. Clinical practice. Asymptomatic primary hyperparathyroidism. N Engl J Med. 2004;350:1746. - PubMed
-
- Brame LA, White KE, Econs MJ. Renal phosphate wasting disorders: Clinical features and pathogenesis. Semin Nephrol. 2004;24:39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
